

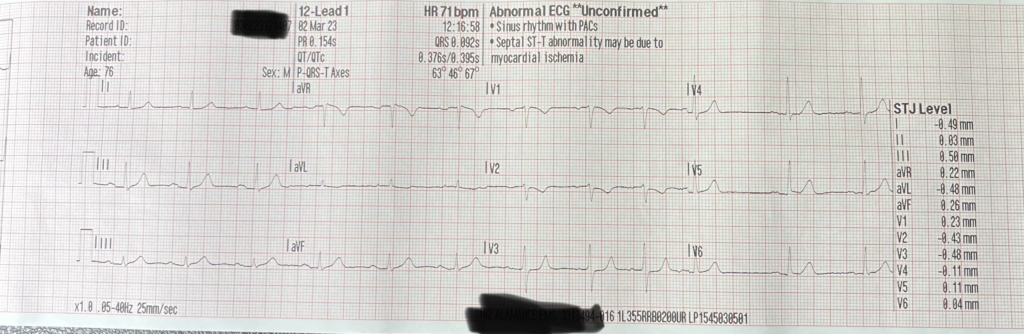
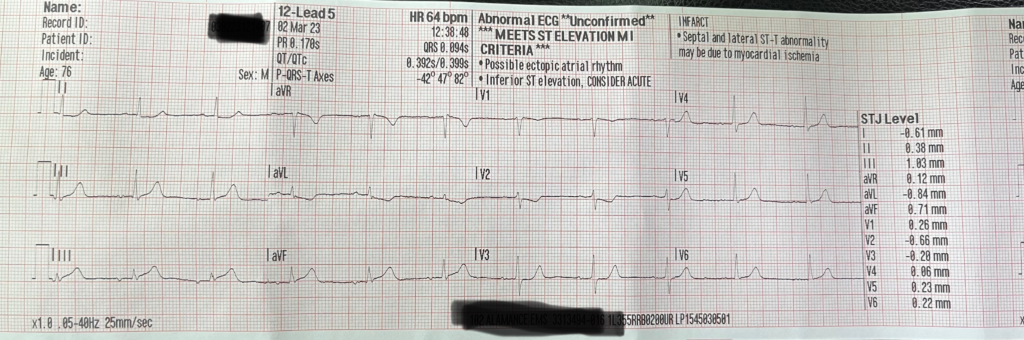
EKGs from the case
Nitroglycerin for acute coronary syndrome.
Nitroglycerin is a medication commonly used to treat acute coronary syndrome, a condition in which the coronary arteries become narrow or blocked, leading to chest pain and other symptoms. Nitroglycerin works by dilating the blood vessels and increasing blood flow to the heart (or so we hoped). It is typically administered in the form of a spray, tablet, or paste; and is primarily used to relieve chest pain.
When it comes to treating acute coronary syndrome, is nitroglycerin an effective medication? Sort of. At the doses we are giving, it likely only dilates the venous system and not the coronary arteries like originally thought. Studies have shown that it can reduce chest pain, but only in 40-50% of cases. It has shown to have a mortality benefit when given IV in the first 24 hours and this is the data we extrapolate to recommend giving sublingual nitro in the field. But even when given IV, the number of patients you would need to treat (NNT) with nitroglycerin to prevent 1 death is somewhere between 125-250. Compared to aspirins NNT in ACS, which is somewhere between 10-42.
There are some important considerations to keep in mind when using nitroglycerin for acute coronary syndrome. For example, it should not be used in patients with low blood pressure (<90mmhg systolic) or in combination with other phosphodiesterase inhibitors such as viagra or Cialis as it can cause an additive effect and lead to a sudden drop in blood pressure. Be aware that patients with pulmonary hypertension are now commonly being placed on long-acting phosphodiesterase inhibitors, such as sildenafil and tadalafil and so it is important to recognize and ask about these medications before administering nitro. In addition, it should be avoided in patients with aortic stenosis, as it can decrease preload and reduce cardiac output.
Overall, nitroglycerin is an effective medication for treating acute coronary syndrome. It is generally well tolerated and side effects are often short live and respond to supportive treatment. It can be used to relieve chest pain and decrease myocardial oxygen demand. However, it is important to be aware of the potential risks and contraindications.
Want to feel clearer about when a treatment helps, hurts, or just makes us feel useful? Join the Loud & Clear Fellowship to practice sorting evidence from habit so your treatment decisions stay patient-centered under pressure.
Nitro relieves chest pain.
Nitro is often used to treat chest pain, and has been used for many years in the out of hospital, prehospital, and emergency department settings. Nitro works by dilating the blood vessels, and in doing so, decreases preload and may help to dilate coronary arteries (although probably only at high IV doses). Nitro can help to relieve chest pain, and reduce the oxygen demand of the heart.
Anecdotally, patients often report that nitro helps to relieve their chest pain. However, it is important to note that there can be uncomfortable side effects, such as headaches and dizziness.
It is also important to note that nitro is not a diagnostic tool. While it may help to reduce chest pain, it does not necessarily mean that the patient is having a coronary event. Nitro can also help to reduce pain from other causes, such as esophageal spasm or GERD.
Nitroglycerin reduces sympathetic outflow.
Nitroglycerin is a smooth muscle vasodilator that works by decreasing pain and in return sympathetic outflow. This decrease in sympathetic outflow can decrease ventricular wall stress and myocardial oxygen demand.
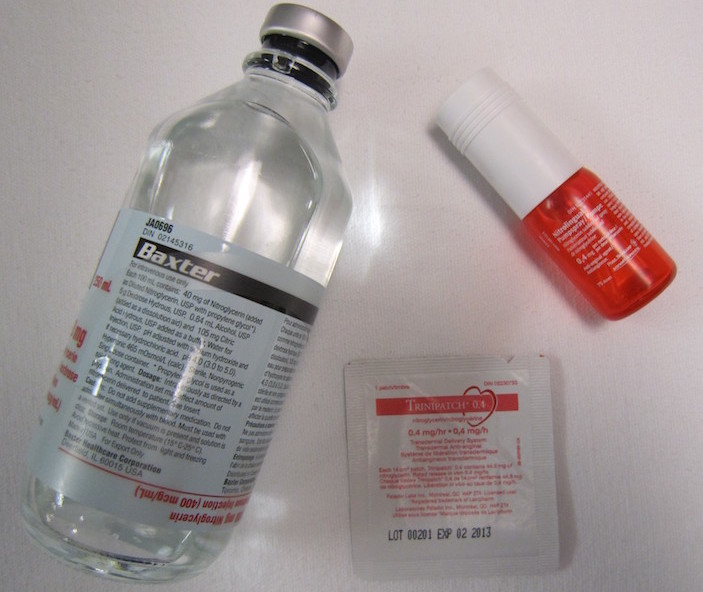
Nitro paste not an ideal treatment in the acute setting
Nitro paste is often touted as an effective treatment for acute coronary syndrome, but it is not the ideal option. The paste is applied directly to the skin, and it takes 10-30 minutes to start seeing the full effect. This is much longer than the five minutes it takes for sublingual tablets and sprays to take effect. So it may not be the best option for patients in the emergent setting or if you have a short transport time. In these cases, sublingual spray or tablets may be a better choice.
Additionally, the paste is dosed in inches, which can lead to a lot of variability in terms of absorption. The sublingual tablets and sprays are the preferred option for treating acute coronary syndrome, as they are much faster and more predictable. They can be used to achieve a peak concentration in less than five minutes, and they have a predictable response. The paste, on the other hand, is meant to provide anginal chest pain relief for up to eight hours. This makes it better suited for long-term use, rather than for treating acute symptoms.
Nitroglycerin and right ventricular MI’s
It is important to consider the potential risks when deciding to use nitro. It has long been feared that inferior right ventricular MIs may be worsened by nitro, as it can decrease preload and potentially lead to hypotension and cardiac collapse. Despite this, recent evidence suggests that nitro is safe to use in these cases, as it has not been found to have a profound effect on hemodynamics. And what effect it does have is generally short lived and responds to a fluid bolus.
Avoid opioids with MI.
When it comes to treating Acute Coronary Syndrome (ACS), the traditional treatment was the MONA protocol: Morphine, Oxygen, Nitro, and Aspirin. However, new evidence has shown that this protocol may not be the best option for treating ACS. Morphine, Oxygen, and Nitro can all have detrimental effects on the patient. Morphine, for example, has been suggested to decrease the effectiveness of anti-platelets, which are essential for reducing mortality. Oxygen has been shown to be toxic and increase ischemic area when titrated to 100%. And nitro can have detrimental effects on your blood pressure.
It is important to be aware of the potential risks associated with the use of opioids in patients with MI. While opioids can be used to reduce pain and decrease sympathetic outflow, they can also have detrimental effects on aspirin absorption. Aspirin, on the other hand, is the only treatment that has been shown to consistently reduce mortality with a low NNT. Therefore, it is important to be cautious when using opioids, such as fentanyl or morphine, as they can delay gastric emptying and absorption of aspirin.
Opioids might be called for in some cases of ACS but it is necessary to weigh the risks and benefits and patient centered goals when considering the use of opioids.
Summary of evidence-based treatment for ACS.
Evidence-based treatment for ACS is a critical component of patient care. Acute coronary syndrome (ACS) is a term used to describe chest pain due to a decrease in blood flow to the heart. It is a serious condition and requires prompt medical attention. The goal of evidence-based treatment for ACS is to reduce the risk of mortality and morbidity associated with the condition.
The most important evidence-based treatment for ACS is the administration of aspirin. Aspirin has been shown to reduce mortality in patients with ACS with a NNT as low as 10.
Nitroglycerin is another evidence-based treatment for ACS. It is used to reduce chest pain and decrease myocardial oxygen demand.
Opioids are also sometimes used for ACS. However, the evidence for their use is not as strong as it is for aspirin and nitroglycerin. Studies have shown that morphine can increase the risk of adverse outcomes in patients with ACS. Therefore, it is important to weigh these risks with specific patient centered goals.
Oxygen saturations in ACS should be titrated to 90-95%. Any higher than this may increase free radicals and lead to a larger area of ischemic injury.
In summary, nitroglycerin is an important medication used in the treatment of Acute Coronary Syndrome (ACS). While it is generally safe and effective, it should be avoided in certain cases, such as patients with hypotension, aortic stenosis, and those taking phosphodiesterase inhibitors.
Want to turn evidence into confident field decisions?
This article challenges an old EMS habit. The Loud & Clear Fellowship helps you keep doing that work with real case discussions, coaching, and practice reps that turn clinical uncertainty into a clear next step.
Citations
Wilkinson-Stokes M, Betson J, Sawyer S. Adverse events from nitrate administration during right ventricular myocardial infarction: a systematic review and meta-analysis. Emerg Med J. 2023 Feb;40(2):108-113. doi: 10.1136/emermed-2021-212294. Epub 2022 Sep 30. PMID: 36180168.
de Alencar Neto JN. Morphine, Oxygen, Nitrates, and Mortality Reducing Pharmacological Treatment for Acute Coronary Syndrome: An Evidence-based Review. Cureus. 2018 Jan 25;10(1):e2114. doi: 10.7759/cureus.2114. PMID: 29581926; PMCID: PMC5866121.
