

In the high-stakes world of emergency medicine, innovations continually push the boundaries of what’s possible. One such groundbreaking procedure is Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA). In this blog post below and the podcast episode with Dr. Ernest E Moore above, we will explore what REBOA is and how it is being used to try and save lives in critical situations. Please note this is an emerging area of trauma resuscitation and as such is actively being studied to best understand if and when it is most beneficial.
Understanding REBOA
REBOA stands for Resuscitative Endovascular Balloon Occlusion of the Aorta. In essence, it’s a medical technique that involves temporarily blocking the aorta using a specialized balloon. This procedure is typically employed when a patient is experiencing severe trauma and concern for uncontrolled bleeding.
The Purpose of REBOA
The primary objective of REBOA is to temporarily control hemorrhage in patients who are in hemorrhagic shock due to severe injuries. The idea is to stop hemorrhage, augment blood pressure, and provide more time for resuscitative efforts and definitive management of the hemorrhagic source.
How REBOA Works
REBOA is usually carried out in a controlled medical environment, often in an operating room or emergency department. Although there are increasing reports of prehospital field use in Europe and the military. Here is a step-by-step breakdown of the procedure:
- Patient Evaluation: The first step is a thorough evaluation of the patient’s condition, including assessing the source and extent of bleeding. REBOA is considered when other methods to control bleeding, such as direct pressure or surgical intervention, are not feasible or have been unsuccessful.
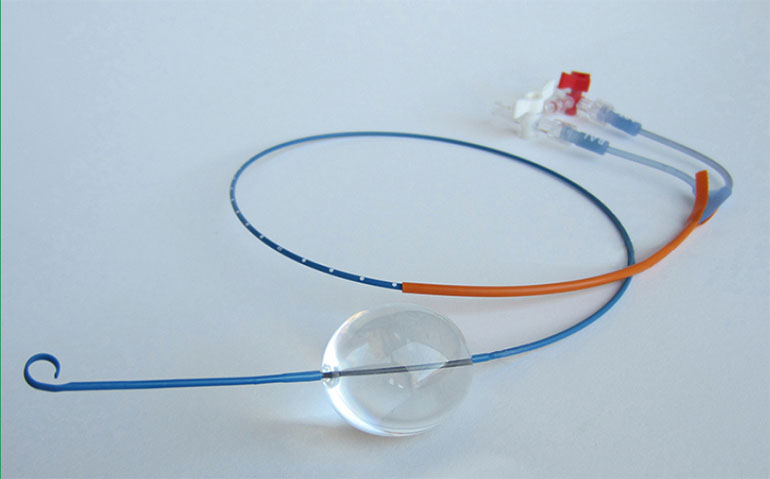
- Balloon Placement: A specialized catheter with a balloon at its tip is inserted into a major artery, typically through the femoral artery in the groin. Using fluoroscopy or ultrasound guidance, the catheter is advanced until the balloon is correctly positioned within the aorta, ideally above the site of injury.
- Balloon Inflation: Once the catheter is properly placed, the balloon is inflated, temporarily blocking blood flow beyond to the injury site. This reduces blood loss and helps stabilize the patient’s condition, buying critical time for further treatment.
- Monitoring: Throughout the procedure, the patient’s vital signs, including blood pressure and oxygen levels, are closely monitored to ensure that the occlusion does not last longer than necessary.
- Deflation and Removal: After the patient is stabilized or when more definitive treatment becomes available, the balloon is deflated, restoring normal blood flow. The catheter is then removed.
The Zones
REBOA has three main zones of placement, each serving a distinct purpose in addressing specific types of injuries and hemorrhages:
- Zone 1 (Proximal Aortic Occlusion):
- Location: Zone 1 is positioned in the segment of the aorta above the diaphragm.
- Purpose: The primary goal of Zone 1 occlusion is to resuscitate the patient while also reducing bleeding from abdominal structures, particularly vascular injuries and liver hemorrhages.
- Common Indications: Zone 1 REBOA is commonly used for severe abdominal and thoracic trauma.
- Time Limit: The maximum recommended time for Zone 1 REBOA occlusion is typically around 30 minutes. Beyond this time frame, there is an increased risk of ischemic complications to vital abdominal organs, particularly the intestines. Prolonged occlusion can lead to bowel and liver ischemia, potentially causing significant irreversible damage.
- Zone 2 (Non-Utilized Area):
- Location: Zone 2 is the area between Zone 1 and Zone 3, starting at the celiac axis (aortic branch supplying the upper abdominal organs) and extending down to the renal arteries.
- Purpose: Zone 2 is considered a “no man’s land” for REBOA placement. It is not typically utilized because occluding this area could compromise blood flow to important organs like the kidneys without providing significant benefits in controlling bleeding. Therefore, REBOA is usually not placed in Zone 2.
- Zone 3 (Distal Aortic Occlusion):
- Location: Zone 3 is located between the renal arteries (supplying the kidneys) and the iliac bifurcation (where the aorta splits into the common iliac arteries leading to the legs).
- Purpose: Zone 3 is primarily used for pelvic fracture hemorrhages. When the balloon is inflated in this area, it can effectively control bleeding from pelvic fractures without significant complications associated with prolonged occlusion.
- Common Indications: Zone 3 REBOA is frequently employed in cases of severe pelvic trauma, where rapid bleeding control is crucial for the patient’s survival.
- Time Limit: Zone 3 REBOA can be used for a more extended duration compared to Zone 1. It may be safely deployed for a more extended period, often beyond 30 minutes. However, the duration of occlusion should still be carefully monitored, and the medical team must assess the patient’s condition and the need for continued REBOA use frequently.
It’s important to note that the choice of REBOA zone depends on the specific clinical scenario and the patient’s condition. Zone 1 is often used when there is a need to address both upper and lower abdominal bleeding, while Zone 3 is reserved for cases of isolated pelvic trauma. The decision on which zone to use is made based on careful evaluation and the patient’s specific needs. Additionally, the duration of occlusion should be closely monitored to prevent complications associated with prolonged blockage of blood flow to vital organs.
Benefits of REBOA
REBOA offers several advantages in critical situations:
- Rapid Hemorrhage Control: It provides a quick and effective means of controlling bleeding, which is crucial in trauma cases where every second counts.
- Minimally Invasive: REBOA is less invasive than open surgical procedures, making it particularly beneficial for unstable patients.
- Bridge to Definitive Treatment: It serves as a bridge to more definitive surgical interventions, allowing time for surgeons to prepare for complex procedures.
Considerations and Risks
While the hope is the use of REBOA can be life-saving, it is not without risks. Prolonged balloon inflation can lead to complications such as organ damage and lower limb ischemia (inadequate blood flow to the legs). Therefore, careful patient selection and monitoring are crucial to minimize these risks.
Conclusion
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) is a remarkable medical procedure that may revolutionize the treatment of severe trauma patients in hemorrhagic shock. By temporarily blocking blood flow to the injured area, the hope is that it will buy time for resuscitation and definitive management of patients in critical condition. While REBOA is not a panacea, its role in modern emergency medicine offers hope to those facing life-threatening injuries, maybe most importantly to those without ready access to a trauma surgeon. We owe a debt of gratitude to medical professionals like Dr. Ernest E. Moore, who tirelessly work to advance these life-saving techniques. You will find his name on most of the literature about REBOA.
Of note, a recent trial was presented at a conference that has gained a lot of publicity on social media. This is the first RCT looking at REBOA vs standard of care. The trial has not been peer reviewed or published yet so should be taken with a grain of salt but here is good a review of what was published at the conference: https://www.stemlynsblog.org/jc-the-uk-reboa-trial-has-the-balloon-popped-st-emlyns/
