
You arrive on scene to find an unconscious patient with pinpoint pupils and slow breathing. You administer naloxone. Nothing happens. The patient remains apneic. What now?
Or consider the agitated, tachycardic patient with dilated pupils who looks like a classic stimulant overdose—except for how warm and overactive they are they’re not sweating at all.
These scenarios aren’t theoretical exercises. This article will teach you the systematic approach to toxicological assessment that works even when you have no idea what substance the patient actually took. You’ll learn to identify the four major toxidromes, understand the critical assessment findings that unlock each diagnosis, and avoid three dangerous diagnostic pitfalls that catch even experienced medics.
Whether you’re a new paramedic building your foundation or a veteran looking to sharpen your skills, mastering toxidromes will transform how you approach overdose calls. The best part? There’s a systematic approach that makes it surprisingly straightforward.
Understanding Toxidromes: Your Diagnostic Framework
A toxidrome combines “toxin” and “syndrome”—it’s a constellation of signs and symptoms characteristic of a class of drugs or poisons. This concept is your secret weapon when patients are unconscious, bystanders are unreliable, or nobody knows what the patient actually took.
Instead of needing to identify the specific drug, you can categorize patients based on physiological findings. From a pathophysiology perspective, toxidromes represent the body’s response to disruption of specific neurotransmitters. Understanding this allows you to predict the clinical course and select appropriate interventions.
Key Insights and Tips:
– Toxidromes provide a systematic approach when you lack definitive information. In most overdose calls, you won’t have reliable information about what the patient took. Toxidromes let you work backward from what you observe to determine the class of substance involved and guide your treatment accordingly.
– Focus on four major toxidromes that represent the vast majority of poisoning presentations. These are sympathomimetic (stimulants), anticholinergic (acetylcholine blockers), opioid (respiratory depressants), and sedative-hypnotic (CNS depressants). Master these four and you’ll be prepared for most overdose calls you encounter.
– Each toxidrome reflects disruption of specific neurotransmitter systems. Sympathomimetics enhance the sympathetic nervous system. Anticholinergics block acetylcholine at muscarinic receptors. Opioids activate mu opioid receptors. Sedative-hypnotics enhance GABA receptors. Understanding the underlying mechanism helps you anticipate what you’ll see clinically.
The Toxicological Assessment: Seven Essential Components
The tox exam differs from your standard medical assessment. It requires specific techniques designed to identify patterns that reveal the toxidrome. Here’s your systematic approach:
Scene Assessment
Look for environmental clues like medication bottles, drug paraphernalia, chemical containers, or unusual odors. Don’t forget: multiple patients with similar symptoms should immediately raise concern for environmental contamination that could affect you.
The emergency department doesn’t have access to the scene or bystanders—you’re their only chance to obtain this information. Be observant and relay what you observe.
Enhanced History Gathering
While the patient may be unreliable, ask bystanders: “Is the patient known to use drugs recreationally?” “Do they have a drug of choice?” “What was the patient doing in the hour before their symptoms started?”
Vital Signs with Temperature
Yes, you take vitals on every patient. But many toxidromes present with characteristic temperature abnormalities that help guide treatment. Heart rate, blood pressure, and respiratory rate are all pieces of the puzzle, but don’t skip the temperature check.
If you don’t carry a thermometer, a simple back-of-the-hand check can suffice. Do they feel super hot or super cold? Pay attention and treat accordingly.
### The Diagnostic Pupil Exam
This is perhaps the most diagnostic single finding in toxicology. Are the pupils big or small? Use proper medical terminology: **mydriasis or mydriatic pupils means big; miosis or miotic pupils means small.**
The key is determining if pupil size is out of proportion to the lighting in the environment. Small pupils in a dark room might be normal. Small pupils in a brightly lit room are significant.
### The Tox Handshake
With a gloved hand, palpate the patient’s axilla (armpit). This provides immediate information about perspiration status. Does your glove come out drenched in sweat or dry as a bone, not a drop of moisture?
**This single finding distinguishes between two toxidromes that otherwise look identical.** We’ll discuss why this matters when we cover sympathomimetic versus anticholinergic toxidromes.
### Neurological Assessment
Focus on consciousness patterns, muscle tone, and clonus. Look for specific patterns:
– Is the patient’s level of consciousness consistent or alternating between sedation and agitation?
– Are they rigid as a backboard or floppy as a sheet?
– If you forcefully dorsiflex the ankle, do they reflexively tap their foot back at you for more than just a few beats? This is clonus.
A patient who is altered or unconscious but stiff as a board is much different than an unconscious patient without muscle tone. The former can be concerning for conditions like neuroleptic malignant syndrome or serotonin syndrome.
### Bowel Sounds
Not something you typically incorporate in your standard medical exam, but different toxins produce characteristic patterns of intestinal activity—hyperactive or hypoactive. This finding can help confirm your clinical suspicion.
**Key Insights and Tips:**
– **Master all seven components of the tox exam to increase your diagnostic accuracy.** Each component provides a piece of the puzzle. When you put them together systematically, the toxidrome becomes clear even when you have no history.
– **The tox handshake and pupil exam are your most powerful diagnostic tools.** These two findings alone can often distinguish between toxidromes that otherwise present similarly. Make them part of every overdose assessment.
– **Document scene findings thoroughly because the ED can’t access this information later.** Your scene assessment and bystander interviews are the only opportunity to gather environmental clues and timeline information that may be crucial for definitive care.
## Sympathomimetic Toxidrome: When Everything Is Turned Up
The sympathomimetic toxidrome results from substances that enhance your sympathetic nervous system. Think of it as everything being turned up to maximum: hyperactive heart, brain, temperature, pupils, sweat glands, and bowels.
### Six Classic Presentations
**Cardiovascular hyperactivity** includes tachycardia often exceeding 120 beats per minute, hypertension with systolic greater than 150 and diastolic greater than 90, and potential dysrhythmias.
Cocaine deserves special mention because it can cause sodium channel blockade that widens your QRS until the rhythm decompensates. This unique finding gets treated with sodium bicarbonate until that QRS narrows.
**Neurological excitation** presents as agitation, hypervigilance, anxiety, and in severe cases, paranoid psychosis with delusions.
**Hyperthermia** shows elevated body temperature due to increased metabolic rate and muscle activity. This is critical because **hyperthermia is the number one predictor of mortality in sympathomimetic overdose.**
**Mydriasis** means pupil dilation out of proportion to the lighting, typically in the range of 6 to 8 millimeters.
**Diaphoresis** is absolutely critical. In a sympathomimetic overdose, these patients are **sweating profusely.** If they’re not—if they’re bone dry—you’re dealing with a different toxidrome likely anticholinergic.
**Gastrointestinal hyperactivity** produces hyperactive bowel sounds due to increased intestinal motility. This is another distinguishing feature between sympathomimetic and anticholinergic toxidromes.
### Common Substances
The three most common substance classes causing sympathomimetic toxidrome are amphetamines (including methamphetamine, MDMA, and therapeutic stimulants), cocaine (with its unique cardiac risks), and synthetic stimulants (including bath salts and novel psychoactive substances).
### Treatment Principles
**Principle one: Benzodiazepines for sedation.** Lorazepam 2 to 4 milligrams IV or midazolam 5 to 10 milligrams IM assists in shutting down the sympathetic nervous system.
**Principle two: Aggressive temperature management.** While hyperthermia is the number one predictor of mortality, it’s unlikely the temperature itself that kills them. This is just a sign that the metabolic system is still out of control and in overdrive. How do you shut that down? Refer to principle one—benzodiazepines.
If the overdose is severe enough that the patient remains hyperthermic, tachycardic, and hypertensive despite usual doses of benzodiazepines, don’t be surprised. **In severe overdoses, these patients often require whopping doses of benzos.** Don’t be afraid to call medical control for additional doses above your protocols until vital signs start to normalize.
**Principle three: Sodium bicarbonate for QRS widening.** If you see QRS widening or a tall R wave in aVR, think cocaine overdose and sodium channel blockade. Give sodium bicarbonate until that QRS narrows.
**Key Insights and Tips:**
– **Diaphoresis is the critical distinguishing feature of sympathomimetic toxidrome.** If you see an agitated, tachycardic patient with dilated pupils who is soaked with sweat, you’re dealing with a sympathomimetic. If they’re bone dry, it’s anticholinergic—a completely different toxidrome requiring different considerations.
– **Don’t be timid with benzodiazepine dosing in severe sympathomimetic overdoses.** These patients may need doses far exceeding your typical protocols. The goal is to shut down the sympathetic overdrive that’s causing the hyperthermia and cardiovascular stress. You’re treating an overdose with an overdose.
– **Hyperthermia is a sign, not the primary problem.** While you can try external cooling measures if time allows, this shouldn’t be your primary focus. The hyperthermia is just a manifestation of ongoing sympathetic overactivation. Shut down the sympathetic system with benzodiazepines and the temperature will follow.
**Common Mistakes to Avoid:**
– **Assuming all agitated, tachycardic patients with dilated pupils are sympathomimetic overdoses.** If the patient isn’t sweating, you’re dealing with an anticholinergic toxidrome. The treatment is mostly the same (benzodiazepines), but you want to avoid antipsychotics like droperidol or haloperidol, which have anticholinergic properties and can worsen anticholinergic toxicity.
– **Focusing too much on external cooling and not enough on sedation.** External cooling is fine if time allows, but the real treatment is shutting down the metabolic overdrive with benzodiazepines. That’s what will actually save the patient.
## Anticholinergic Toxidrome: Mad, Red, Dry, Blind, and Hot
The anticholinergic toxidrome results from blockade of the parasympathetic nervous system, which relies on the neurotransmitter acetylcholine. The parasympathetic system is meant to counterbalance the sympathetic. When you lose that counterbalance, you experience a very similar effect to sympathomimetic toxicity—but with one big difference and some subtle other differences.
### The Five-Component Mnemonic
**Mad as a hatter:** Altered mental status ranging from mild confusion to frank delirium with visual hallucinations. Here’s how to distinguish this from sympathomimetic agitation: If they’re screaming at you and you can make out every profanity clearly, it’s likely sympathomimetic. If it’s a bunch of gibberish that makes no sense at all, it’s likely anticholinergic.
**Red as a beet:** Characteristic flushed erythematous skin due to vasodilation. This will be even more pronounced than what you’ll see with stimulants.
**Dry as a bone:** This is the critical difference. The tox handshake reveals **complete absence of sweating despite hyperthermia.** Sweat glands are controlled by the M3 muscarinic receptor and require activation by acetylcholine to induce perspiration. This is blocked in anticholinergic overdose but unaffected by sympathomimetic overdose.
**Blind as a bat:** Mydriasis with pupils often 8 millimeters or greater.
**Hot as hell:** Severe hyperthermia that can be life-threatening because **these patients cannot cool themselves through perspiration.**
### Common Sources
The four most common sources are antihistamines (particularly diphenhydramine in recreational or overdose situations), tricyclic antidepressants (rarely used anymore but can have profound anticholinergic effects), antipsychotic medications (in intentional overdoses or therapeutic dosing errors), and plant sources (jimson weed, nightshade, and other botanical intoxications).
### Treatment Interventions
**Intervention one: Benzodiazepines.** This is your mainstay of therapy. Titrate to both agitation and abnormal vital signs. Lucky for us, this is the same dosing as sympathomimetic toxidrome. So even if you think it’s sympathomimetic when it’s actually anticholinergic, benzos are still the primary treatment.
However, antipsychotics such as droperidol may be safe and effective for controlling agitation in sympathomimetic overdose, but **they can actually have significant anticholinergic properties and worsen an anticholinergic toxidrome.** If you’re unsure between the two toxidromes, stick with benzos.
**Intervention two: Aggressive external cooling** for any hyperthermia because the acetylcholine blockade at sweat glands prevents these patients from regulating their own temperature with perspiration.
**Intervention three: Urinary catheterization** when retention is present. The smooth muscles of the bowel and bladder rely on acetylcholine activation. Anticholinergic toxicity leads to smooth muscle paralysis, causing urinary retention. Think back to the last time you held your bladder too long—did you have much patience for questions? That’s exactly what these patients may be experiencing. **Draining the bladder often drastically improves agitation.**
**Intervention four: Physostigmine** may be considered but only in severe cases of pure anticholinergic toxicity refractory to benzodiazepines. Physostigmine is an anticholinesterase inhibitor that prevents breakdown of acetylcholine at the nerve synapse, increasing its concentration to overcome the anticholinergic blockade. However, this is the exact same mechanism as organophosphate poisoning and can lead to dangerous complications. It’s not first-line therapy, and rescue agents like atropine should be at bedside if it’s used.
**Key Insights and Tips:**
– **The toxicological handshake is your key to distinguishing anticholinergic from sympathomimetic toxidrome.** Sympathomimetic patients are soaked with sweat. Anticholinergic patients are bone dry.
– **Bowel sounds provide additional confirmation.** Sympathomimetics cause hyperactive bowel sounds due to increased intestinal motility. Anticholinergics cause hypoactive bowel sounds due to smooth muscle paralysis. Listen to the abdomen as part of your assessment.
– **Consider urinary retention as a cause of agitation.** If you see ongoing hyperactivity and agitation despite adequate doses of sedatives and improvement in vital signs, the patient may have a painfully distended bladder. Draining it can dramatically improve their mental status.
**Common Mistakes to Avoid:**
– **Using antipsychotics for agitation in anticholinergic toxidrome.** Medications like droperidol and haloperidol have anticholinergic properties themselves and can worsen the toxicity. Stick with benzodiazepines for sedation.
– **Relying solely on external cooling for hyperthermia.** While external cooling helps, remember these patients can’t thermoregulate through sweating. You need to address the underlying anticholinergic blockade with benzodiazepines to shut down the metabolic overdrive causing the hyperthermia.
## Opioid Toxidrome: The Classic Triad and Its Dangerous Impostor
The classic opioid toxidrome represents three cardinal features: CNS depression (from somnolence to complete unresponsiveness), respiratory depression (the life-threatening component with decreased rate and shallow breathing), and miosis (pinpoint pupils out of proportion to lighting, typically 1 to 2 millimeters).
But there’s a dangerous impostor that presents with identical features and can fool even experienced medics. More on that below.
### Opioid Classes
Opioids are broken into three classes. Natural opioids (also called opiates) like morphine, codeine, and opium are made from opium poppy plant seed pods. Semi-synthetic opioids like heroin, oxycodone, hydrocodone, and hydromorphone are made in laboratories by chemically processing natural opioids. Synthetic opioids like fentanyl and carfentanil are manufactured entirely in laboratories with no natural ingredients.
Generally, the more synthetic the opioid, the more potent it is.
### Three Essential Naloxone Principles
**Principle one (most important): The goal is respiratory restoration, not full consciousness.** This principle informs everything else about naloxone administration.
**Principle two: Start with 0.4 to 0.5 mg and titrate to breathing, not alertness.** You want to restore adequate respiratory effort, not wake the patient up completely.
**Principle three: Reserve 2 milligram slugs for cardiac arrest or peri-arrest only.** Recent research suggests naloxone may improve neurologically intact survival in cardiac arrest, though the evidence is limited.
### Why Judicious Dosing Matters
If you give too much naloxone too fast, you can precipitate a withdrawal syndrome that can include vomiting and agitation—no fun for anyone involved. **A breathing but sleeping patient is much easier and safer to care for than an agitated, vomiting patient.**
There’s also a rare but serious complication of flash pulmonary edema. The mechanism isn’t well understood, but one leading theory is that naloxone induces a big forceful respiration against a closed glottis, creating such negative intrapulmonary pressures that it causes a massive shift of fluids from the vasculature into the lungs. If this occurs, management is noninvasive positive pressure ventilation titrated to hypoxia and work of breathing.
### The Dangerous Impostor: Alpha-2 Agonists
What happens if you give repeat doses of naloxone totaling 2 to 4 mg and you’re not seeing any correction of respiratory depression? **Alpha-2 agonists like clonidine cause identical presentations—unconsciousness, respiratory depression, and pinpoint pupils—with the hallmark being lack of response to naloxone.**
Fail to recognize this and your patient dies while you’re wondering why naloxone isn’t working. The fix is airway management. **Support their respirations with mechanical ventilation until the drug wears off.**
In alpha-2 agonist overdoses, you may also see profound bradycardia and hypotension. This gets managed supportively with vasopressors like epinephrine drip, which increases heart rate through beta-1 receptors in the heart and vascular tone through alpha-1 receptors in the arterioles.
**Key Insights and Tips:**
– **Titrate naloxone to respiratory effort, not consciousness.** Your goal is a patient who is breathing adequately on their own, even if they remain sleepy. Overshooting this goal creates unnecessary complications like withdrawal, agitation, and vomiting.
– **Start low and go slow with naloxone dosing.** Beginning with 0.4 to 0.5 mg allows you to restore breathing without precipitating withdrawal. You can always give more if needed, but you can’t take it back once given.
– **If naloxone doesn’t work after appropriate dosing, consider alpha-2 agonists.** Clonidine and similar sympatholytic agents present identically to opioid overdose but don’t respond to naloxone. The key differential point is lack of improvement after naloxone. Switch to supportive airway management and consider vasopressors if needed.
**Common Mistakes to Avoid:**
– **Giving large naloxone boluses to “wake up” the patient.** This precipitates withdrawal and creates an agitated, potentially violent patient who may also be vomiting. It doesn’t improve outcomes and makes your job much harder.
– **Assuming all unconscious patients with pinpoint pupils are opioid overdoses.** Alpha-2 agonists like clonidine create an identical presentation. If naloxone doesn’t work, switch to airway management and supportive care.
– **Missing the additional clues of alpha-2 agonist overdose.** While the presentation mimics opioids, these patients often also have bradycardia and hypotension, which are less common with pure opioid overdose. These additional findings should raise your suspicion.
## Sedative-Hypnotic Toxidrome
Sedative-hypnotic toxidrome presents with four key characteristics that distinguish it from opioid toxidrome: CNS depression with preserved respiratory drive (unless the overdose was massive), normal pupils (not pinpoint like opioids), normal respiratory rate (again, unless massive doses or co-ingestions are involved), and stable vital signs with normal blood pressure and heart rate.
### Four Major Drug Classes
**Class one: Benzodiazepines** like alprazolam, lorazepam, and diazepam.
**Class two: Non-benzodiazepine sleep aids** (Z-drugs) like zolpidem.
**Class three: Barbiturates.** Commonly abused recreationally in the 1990s, they’ve been on steady decline and now account for very few single-agent deaths annually. They’re still commonly used as anticonvulsants clinically.
**Class four: Gamma-hydroxybutyrate (GHB).** This is the hidden danger that requires special attention.
### The GHB Exception
Unlike other sedative-hypnotics, **GHB can cause alternating periods of deep sedation with sudden violent agitation.** One moment your patient is unconscious, the next they’re combative and potentially dangerous to you and your entire crew.
When we say deep sedation, we mean deep sedation. These patients may have periods of apnea. Generally, these apneic episodes are short-lived, and if you can briefly support them through it, it will self-resolve. Occasionally, however, you do have to intubate them.
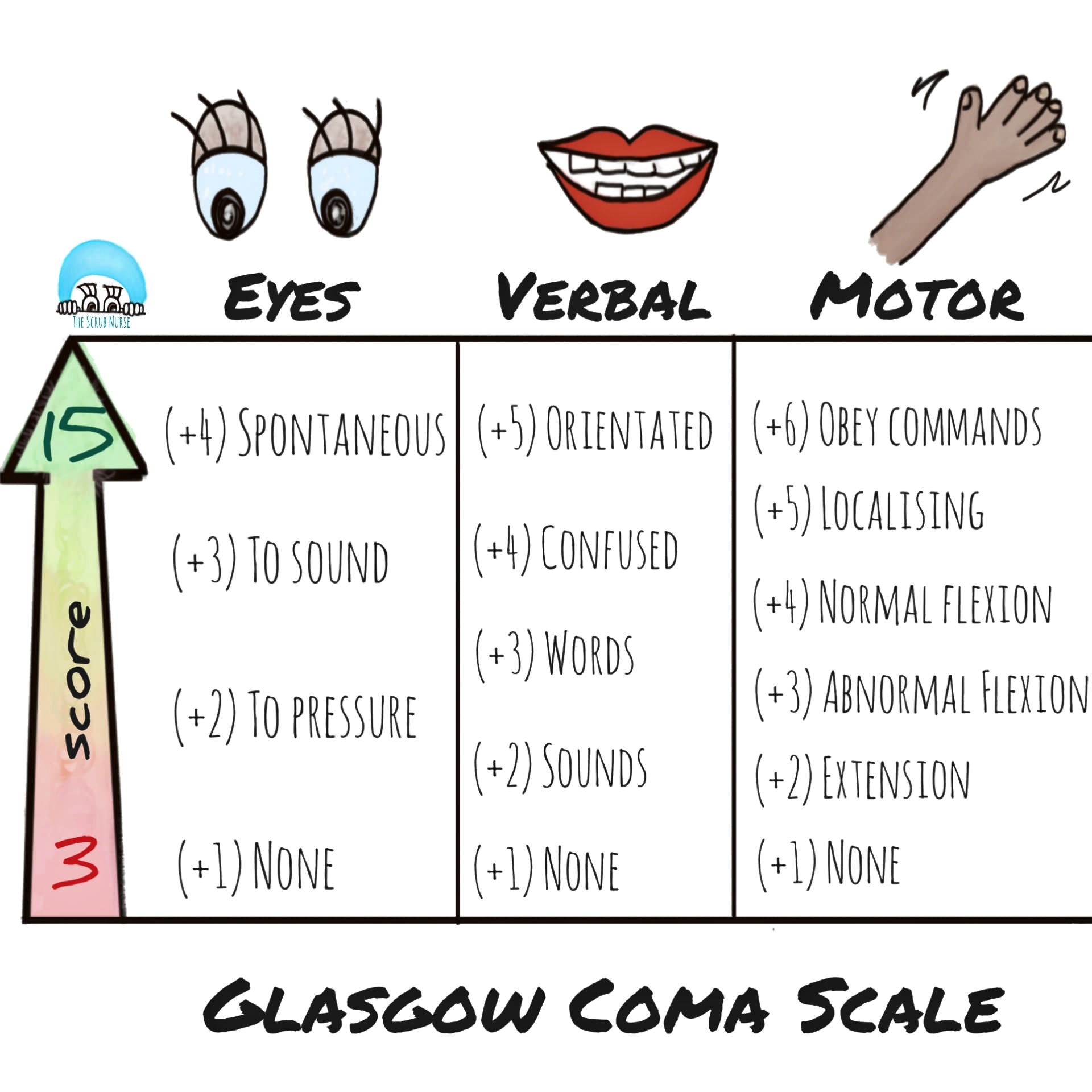
The challenge is the unpredictability. A patient can go from completely unconscious (GCS of 3) to suddenly sitting up, kicking, and screaming, then back to unconscious again—all within seconds.
### Three-Point Management Approach
**Point one: Airway management** with positioning and adjuncts as needed.
**Point two: Supportive care.** Mechanical ventilation is rarely required. Airway and breathing are your biggest risks with sedative-hypnotics, but problems are rare and usually only happen in large ingestions or co-ingestions.
**Point three: Consider flumazenil** (the antidote for benzodiazepines), but it carries significant risk and is rarely used or recommended. It can precipitate seizures in benzodiazepine-dependent patients, and its duration of action is shorter than many benzodiazepines, leading to re-sedation when it wears off.
Really, the biggest thing is airway management, supportive care, and allowing the medicine of time to metabolize the drug.
**Key Insights and Tips:**
– **Normal pupils and normal respiratory rate distinguish sedative-hypnotic from opioid toxidrome.** This is your key differential point. Opioids cause pinpoint pupils and respiratory depression. Sedative-hypnotics cause normal pupils and usually preserve respiratory drive unless the overdose is massive.
– **Be prepared for sudden violent agitation with GHB.** Unlike other sedative-hypnotics that cause predictable sedation, GHB can cause wild swings between deep unconsciousness and combative agitation. Position yourself safely and have a plan for rapid chemical or physical restraint if needed.
– **Flumazenil exists but is rarely indicated.** While there’s an antidote for benzodiazepines, the risks often outweigh the benefits. It can cause seizures in dependent patients and wears off faster than the benzodiazepine, leading to re-sedation. Supportive care is usually the better approach.
**Common Mistakes to Avoid:**
– **Assuming all sedative overdoses will remain sedated.** GHB is the exception that can suddenly become violent. Maintain situational awareness and don’t let your guard down just because the patient appears unconscious.
Five Essential Clinical Pearls for Exceptional Practice
Pearl One: Master the tox handshake. Sweating status instantly differentiates sympathomimetic from anticholinergic toxidrome. This single assessment finding can change your entire diagnostic approach.
Pearl Two: Pupil size is relative to the environment. Focus on the discrepancy—pupils that are larger than expected for a bright environment or smaller than expected for a dark environment. Normal pupil size varies, so context is everything.
Pearl Three: Your naloxone goal is breathing, not consciousness. Titrate to respiratory effort, not wakefulness. Start with 0.4-0.5 mg and increase slowly. A breathing but sleeping patient is much easier and safer to care for than an agitated, vomiting patient in withdrawal.
Pearl Four: Be prepared for mixed ingestions that may be unmasked by your initial treatment. Full and continuous cardiorespiratory monitoring is essential because these patients can deteriorate rapidly once you’ve addressed one component of their toxidrome.
Pearl Five: Chemical sedation is superior to physical restraint in most cases. For patient safety with agitated toxidrome patients, use benzodiazepines as your first-line intervention. If physical restraints become necessary, avoid positional asphyxia and maintain continuous monitoring.
Final Thoughts: From Competent to Exceptional
The difference between competent and exceptional medics lies in pattern recognition and systematic assessment. You now have both tools at your disposal.
Toxidromes provide a systematic approach to poisoning when specific agents are unknown. Master these patterns and you’ll provide evidence-based care even in the most challenging toxicological emergencies. The beauty of this approach is that it works backward from what you observe to guide appropriate treatment, even when patients are unconscious, bystanders are unreliable, or nobody knows what was actually taken. All you have to do is react to the signs and symptoms you’re seeing in front of you.
Remember, during acute resuscitation, you often don’t need to know the specific drug. You need to recognize the pattern, understand the underlying pathophysiology, and respond with appropriate toxidrome-specific interventions. Start with the seven-component tox exam, identify the toxidrome, and follow your systematic algorithm.
The next time you arrive on scene to find an unconscious patient with unclear ingestion history, you’ll have the framework to provide exceptional care based on what you can observe rather than what you can’t know.
