


Want to get faster at recognizing medication toxicity before the picture is obvious? Inside the Loud & Clear Fellowship we practice spotting subtle clues and building a treatment plan when the history is incomplete.
Serotonin Toxicity
Serotonin Toxicity is a spectrum. Early recognition and treatment is key to preventing bad outcomes.
Typically seen in patients who have overdosed on party drugs like MDMA, ecstasy, Molly etc. Also seen in patients on multiple medications that increase serotonin levels. Most antidepressants increase serotonin levels. Be suspicious of serotonin syndrome in a patient with signs and symptoms who recently had medications changed or added.
Hyperthermia is what kills–serotonin increases muscle activity = heat
#1 predictor of mortality is temperature
Untreated serotonin toxicity leads to the final common pathway of most toxicological emergencies: seizure > coma > death.
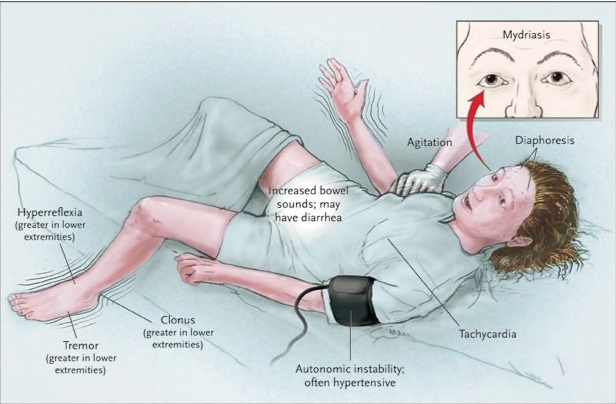
Signs and Symptoms:
Clonus Video:
https://youtu.be/1X-br14gCVoOcular clonus video
https://youtu.be/oAOO5y68O-U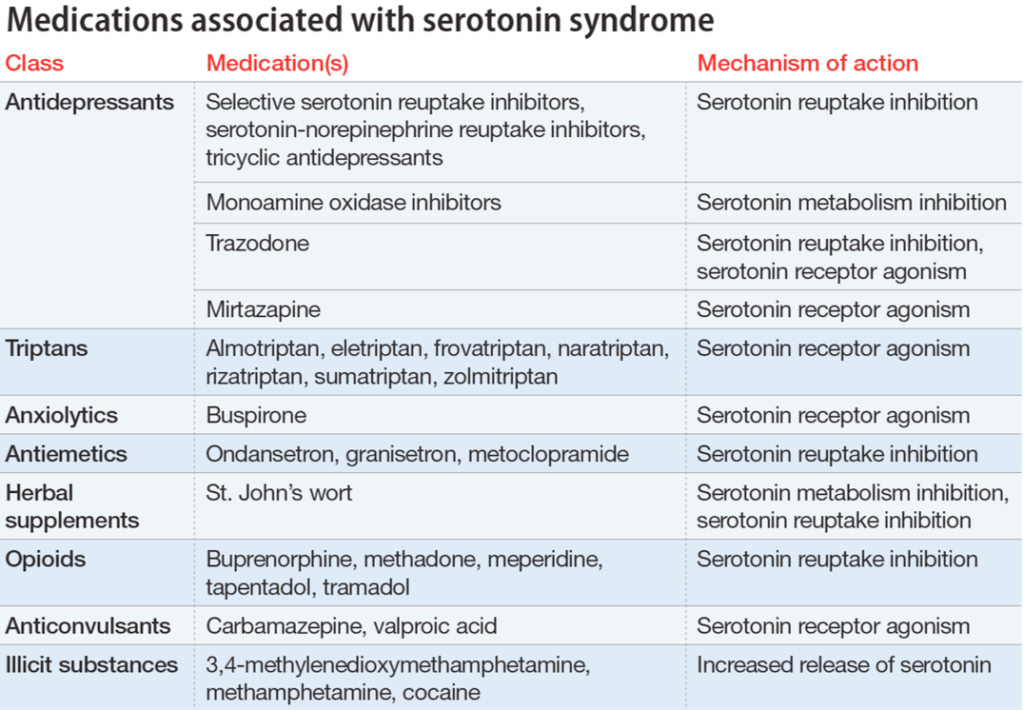
Differential Diagnosis
- Neuroleptic Malignant Syndrome – more gradual, usually related to dopaminergic meds like antipsychotics or medications used to treat patients with Parkinson’s disease
- Malignant hyperthermia – almost always associated with exposure to anesthetics or paralytics
- sympathomimetic toxicity – also causes increased HR, BP, agitation but less likely to see sustained clonus
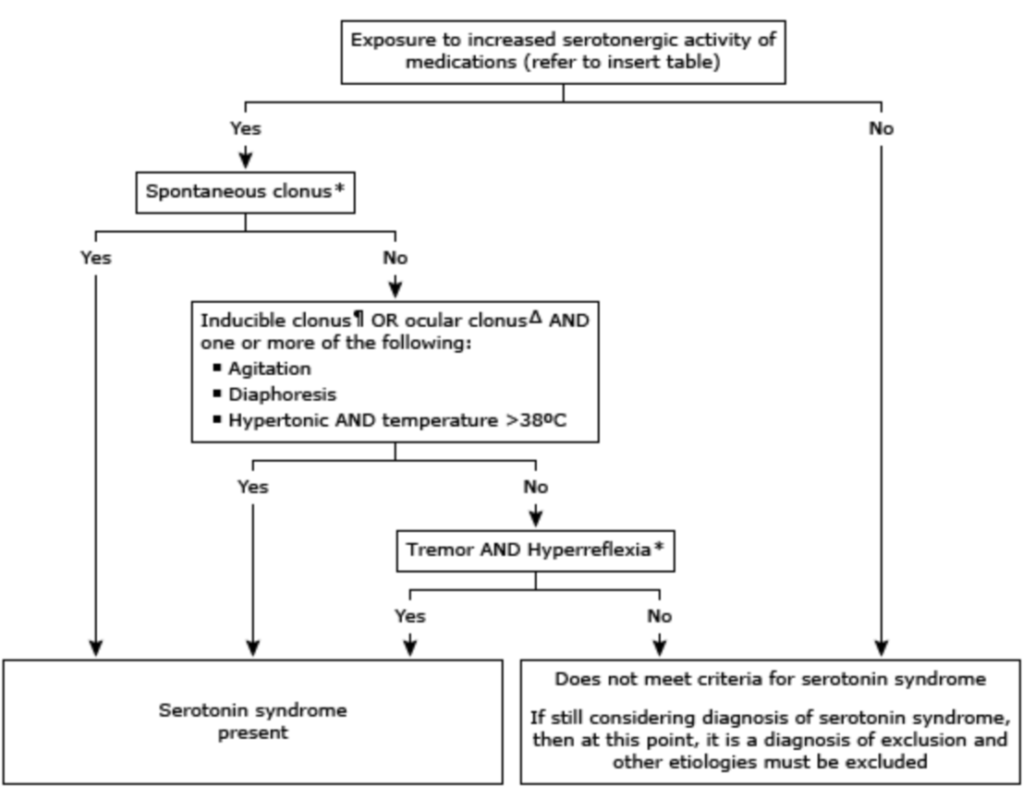
Diagnosis of serotonin syndrome is a clinical diagnosis meaning it is made based on history, signs, and symptoms and not with a lab test or imaging study. Below are the Hunter Criteria Nik talks about in the show laid out in algorithm format:
Treatment:Benzodiazepines are the mainstay of treatment – way more than you’re used to giving. Keep giving it until hyperthermia resolves or you need to intubate them. Even if they are sedated keep giving if they are still hot. This will save their life.Don’t be afraid to call med control for high and repeat doses of benzos. There is no maximum dose. External cooling is helpful but do not delay benzo administration to perform cooling measures. Cooling is best done with evaporative cooling: Take a sheet and use saline or water to get the entire sheet soaked. Place the wet sheet over the naked patient and fan them (windows down if needed)Ice packs are less effective but can be used if available. If you need to intubate these patients try to avoid succinylcholine for RSI and use rocuronium instead when choosing a paralytic. For induction, use etomidate if available. Avoid using opioids as they can be serotonergic.
Want help turning subtle tox clues into a clear plan?
This article gives you the clinical pattern. The Loud & Clear Fellowship gives you practice applying patterns like this to realistic calls, so uncertainty becomes a focused next step.
