


- **CORRECTION** In the summary at the end of part 1, the rule of 5’s was inappropriately attributed to the pediatric population. Rule of Fives is meant for morbidly obese adults, not for kids. Lund-Browder is great tool for peds of different age ranges, though still doesn’t address body morphology (obese kids). Resource- Evaluation and Optimization of the Wallace Rule of Nines for the Estimation of Total Body Surface Area in Obese and Nonobese Populations, The Journal of Emergency Medicine, Volume 65, Issue 4, 2023, Pages e320-e327.
Burn Injuries
These are among the most intimidating emergencies faced by prehospital care providers. The intricacies of managing such cases were vividly discussed in our recent podcast featuring Derek Miller, an experienced burn nurse with a deep understanding of burn care. This post delves into the key takeaways from the podcast, offering practical guidance and insight to enhance the care of burn patients in the prehospital setting.
The Burn Life Threats
Burn patients are unique due to the multifaceted nature of their injuries, which can often mask other life-threatening conditions. For instance, a burn might distract from underlying traumas or inhalation injuries, necessitating a thorough trauma assessment to ensure nothing is missed. Derek emphasizes the importance of considering polytrauma, airway compromise, and other types of shock that might accompany or even overshadow the burns themselves. The most important first step in a burn patient is to assess for and address, what Derek refers to as, the big 3 life threats-
- Traumatic injuries and other flavors of shock- burns are often associated with polytrauma. This will kill the patient long before the burn does. Don’t be distracted by the burn, treat trauma like you know how to treat trauma. Address traumatic injuries like you would in any other trauma patient. Also be aware of other flavors of shock that may be less intuitive but also can present in association with a burn. Examples- 1. a farmer uses gasoline to burn a nest of bees, suffers 3rd degree burns to legs, but also suffers anaphylaxis from dozens of bee stings on top of the severe burn, 2. Delay in presentation for the poorly compliant diabetic with neuropathy who burns foot but only calls 911 and goes to ER a few days later with a raging cellulitis + septic shock, 3. Cardiogenic shock from arrhythmias secondary to electrical injury or hydrofluoric acid exposure (resulting in hypocalcemia). Point being the hypoperfusion/hypotension is LIKELY classic trauma BUT could also be due to less conventional forms of shock.
- Airway compromise- From trauma or the burn itself which can lead to a significant amount of airway swelling and edema. Mucosal burns can lead to a significant amount of edema especially with time as the capillaries become more leaky and fluid starts to third space. Be on the lookout for any worsening edema and treat early if concerns for imminent airway loss exist.
- Inhalation injury- Burn inhalation can lead to direct alveolar damage impairing the lungs ability to preform gas exchange. This will often respond to oxygen and noninvasive positive airway pressure. Also be on the lookout for possible toxic inhalations such as carbon monoxide or cyanide poisonings. For specifics on how to treat these refer to Ep. 19: Carbon Monoxide and Ep. 39: Cyanide.
Types of Burns:
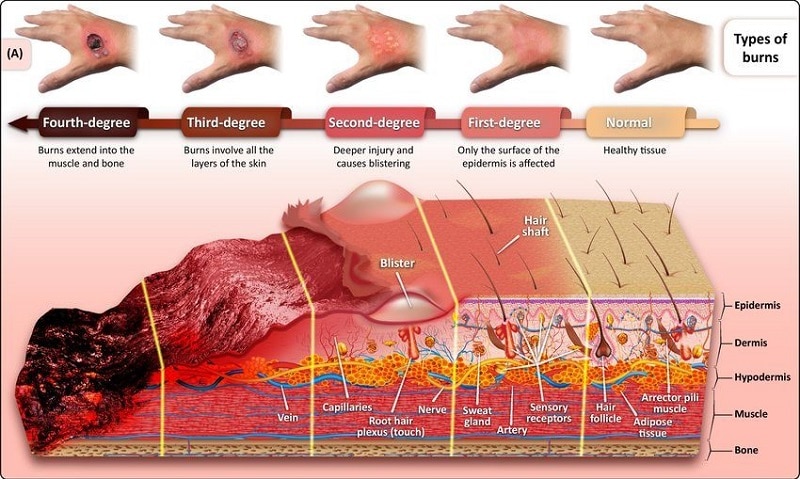
- First-Degree Burns (Superficial): Affect only the epidermis, causing redness and pain but generally healing without permanent damage.

- Second-Degree Burns (Partial Thickness): Extend into the dermis, causing intense pain, swelling, and blistering. These burns may heal with care but can leave scarring.

- Third-Degree Burns (Full Thickness): Penetrate the full thickness of the skin, destroying both the epidermis and dermis, and possibly affecting underlying tissues. These burns often require surgical intervention and can lead to significant functional and cosmetic deficits.

- Fourth-Degree Burns: Extend beyond the skin into muscles and bones, often resulting in catastrophic outcomes.
Initial Estimate of Burn Size
When estimating total body service area burned (TBSA), remember only second and third degree burns count. 1st degree burns which look just like a sun burn do not get calculated in our TBSA. There are two down and dirty methods for estimating TBSA in the prehospital setting. But first you’re going to want to make sure the patient is completely exposed so your not missing any areas or secondary trauma.
Here is a link from ABA that may be helpful, it includes a brief overview of severity/depth (with diagrams, not pictures), Rule of Nines & Palmar Method, plus a link for ABA referral criteria.:
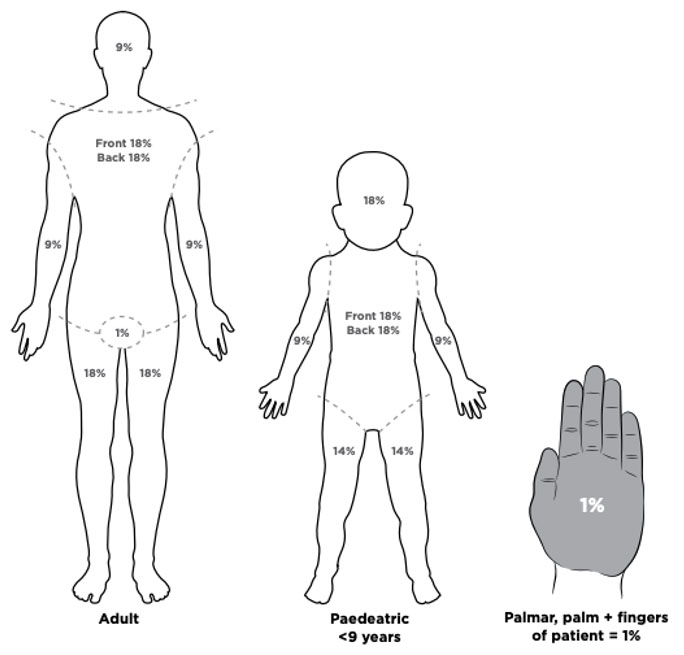
- Rule of 9’s – If the burn is very large and involving whole body parts you’re going to want to use the rule of 9’s realizing this is adult centric and for a pediatric patient more weight is given to the head and less to the legs.
- Palmar Surface – If the burn is very patchy and doesn’t involve the entire extremity, the palmar surface rule will be easier, quicker, and involve less math. The palmar surface rule refer to the size of the patients palm, including the fingers that are closed without space in-between them. This area, an area the size of the patients palm, correlates with approximately 1% of TBSA.
Here is another great article for a deeper dive into pros & cons of different methods of estimating TBSA.
- Gretchen J. Carrougher, Tam N. Pham, Burn size estimation: A remarkable history with clinical practice implications,Burns Open, Volume 8, Issue 2, 2024, Pages 47-52, ISSN 2468-9122.
Critical Burn Threshold
Once we have an idea of the total area, roughly 20% is going to be that threshold that we consider a critical burn. This is the point at which you not only have a local tissue inflammatory response but may experience a systemic inflammatory response that will lead to capillary leak and significant fluid losses.
Fluid Resuscitation
Fluid resuscitation is critical in burn care. But is also a fine balance. Studies have demonstrated that most burn patients involve over-resuscitated with fluids not under-resuscitated, which can be just as detrimental. When we’re thinking about fluid replacement needs for the patient the modified Brooke and the Parkland formula are the two most commonly referenced methods.
2-4ml x Weight (kg) x TBSA = Estimated fluid needs in first 24 hours
This calculation gives us the expected fluid loss in the first 24 hours with most of that occurring in the first 8 hours. But remember this takes hours to develop and occur. And while it is important to stay ahead of these fluid losses. Most burn patients tend to be over resuscitated and not under resuscitated and the amount of fluids we start prehospitally tend to get continued in the hospital so we need to be careful.
In addition, this formula involves a carnival trick in attempting to guess the patients weight and then preforming math equations while you’re dealing with a critical patient. It’s just not set up for success in the prehospital setting. In part 2 we’ll get into a simpler fluid administration strategy but for now, realize these patients don’t need a lot of fluids up front from us. If they are hypotensive, then yes by all means, fluid bolus but realize it’s not the burn making them hypotensive and search for another underlying etiology that you can treat.
An overview of evolution of burn fluid resuscitation formulas & philosophy can be found in this paper.
- Bacomo, F. K., & Chung, K. K. (2011). A primer on burn resuscitation. Journal of emergencies, trauma, and shock, 4(1), 109–113. -Key concept here is Ivy Index (aka, exceeding 250mL/kg of fluids in 24h). For large burns, exceeding 8oz of fluid/kg over a 12h span is scary predictor of mortality.
Another article demonstrates that “fluid begets more fluid”. In actual practice nearly everyone gets substantially more than formula predicts. And this article underscores the risks of fluid creep. Starting too high, being reluctant to titrate down, and the fact that giving too much fluid can actually CAUSE an increased need for fluids (vicious cycle).
- Chung KK, Wolf SE, Cancio LC, Alvarado R, Jones JA, McCorcle J, King BT, Barillo DJ, Renz EM, Blackbourne LH. Resuscitation of severely burned military casualties: fluid begets more fluid. J Trauma. 2009 Aug;67(2):231-7; discussion 237. doi: 10.1097/TA.0b013e3181ac68cf. PMID: 19667873.
A Better Approach to Fluid Management
Practical Application in Prehospital Settings
For prehospital providers, particularly those infrequently encountering severe burns, the recommendation is to streamline the fluid resuscitation process:
- Initial Rate Setting: For adults (>13 years old) with significant burns, start with a standard rate of 500 ml/hr lactated ringers solution preferred if available, but if not normal saline is fine. Adjustments can be made based on the patient’s response and ongoing assessment.
- Adjustments for Children: Adjust fluid rates for children based on age
- 6-13 years old – 250 ml/hr
- <6 years old – 125 ml/hr
Vascular Access
Vascular access may be especially challenging in these patients depending on area burned or fluid status. Don’t be afraid to reach for intraosseous (IO) access if needed. This can be preformed in awake patients if they are critically ill and IV access is not feasible or unsuccessful.
Pain Management
Addressing pain in burn victims is not just a matter of comfort but a critical aspect of patient management. Effective pain control can facilitate better overall patient management and reduce stress for both the patient and the provider. Studies have also demonstrated that adequate pain control positively effects burn healing and decreases the risk of PTSD. The psycological impact of burn injuries cannot be overstated. Providing pain control, reassurance, and support, explaining actions as you preform them, and maintaining a calm, composed demeanor can help alleviate some of the patient’s distress.
Conclusion
In conclusion, the prehospital management of burn injuries demands a meticulous and systematic approach to ensure optimal outcomes. Identifying life-threatening conditions early, such as airway compromise and shock, is crucial for prioritizing interventions and can be the difference between life and death. Accurately estimating the total body surface area (TBSA) affected by burns is essential for guiding treatment decisions, particularly in fluid resuscitation, which requires a careful balance to avoid complications from both under and over-resuscitation. Remember the fluids you start prehospitally, whether right or wrong, tend to get continued in the hospital. Simplify your approach to fluid resuscitation in these patients. 500ml/hr if <13 years old. 250ml/hr if 6-13 years old. 125ml/hr if <6 years old. This is where we should start with our fluid resuscitation, and will be appropriate for the vast majority of patients, but effective fluid resuscitation in burn patients requires more than just following strict black and white protocols—it demands an understanding of the underlying principles, a readiness to adapt to dynamic situations, and a focus on individual patient needs. By simplifying decision-making processes and utilizing available tools and technologies, prehospital providers can improve outcomes for burn victims, ensuring they receive the best possible care from the point of injury to definitive treatment. Moreover, effective pain management not only alleviates the intense discomfort associated with burns but also aids in overall patient stability and recovery. Each of these aspects underscores the complexity and critical nature of burn care in the prehospital setting, highlighting the importance of the care you provide in the prehospital setting.
