How the aviation industry has revolutionized itself through such methodologies as just culture, crew resource management, and error prevention tools like the inquiry, advocacy, assertiveness
Effective agitated patient management requires a fundamental shift from viewing these encounters as behavioral problems to recognizing them as medical emergencies with underlying pathophysiological processes.
In emergency medicine, few scenarios are as immediately concerning as arriving on scene to find a patient actively vomiting bright red blood. Upper gastrointestinal (GI)
These challenging scenarios represent opportunities to provide truly patient-centered care at life's most vulnerable moments. By combining your medical expertise with thoughtful communication, you can
Let's discuss the intricacies of evidence-based medicine (EBM) with Dr. Ben Li. The conversation dives deep into understanding different types of medical studies, their hierarchies,
Syncope, is a symptom that many emergency medical personnel encounter. It's sometimes tricky to differentiate from seizures, and it's essential to understand that syncope is
Let's discuss the pressing issue of mental health among first responders, particularly within the EMS community. Will gets vulnerable and shares a personal story of
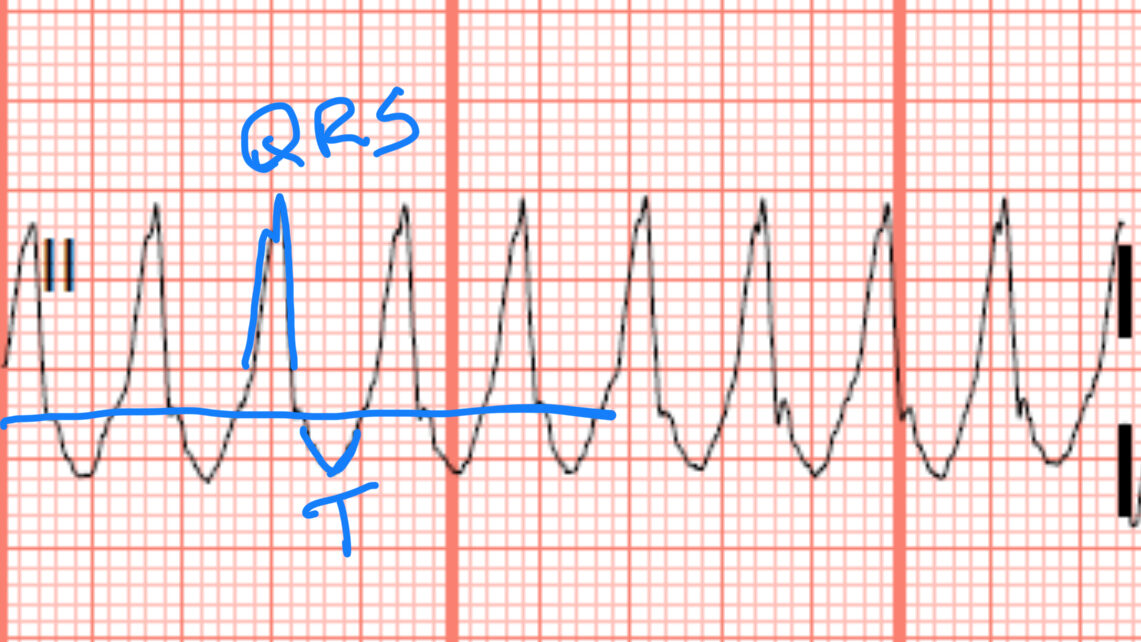
Learn a systematic approach to management of wide complex tachycardia that doesn't rely on exact rhythm identification or scoring systems with guest Dr. Kevin Butler.
Joined by Josh, Cody, and Moose from the AlertMedicOne podcast, we explore key principles of good training, leadership, and the importance of making mistakes in
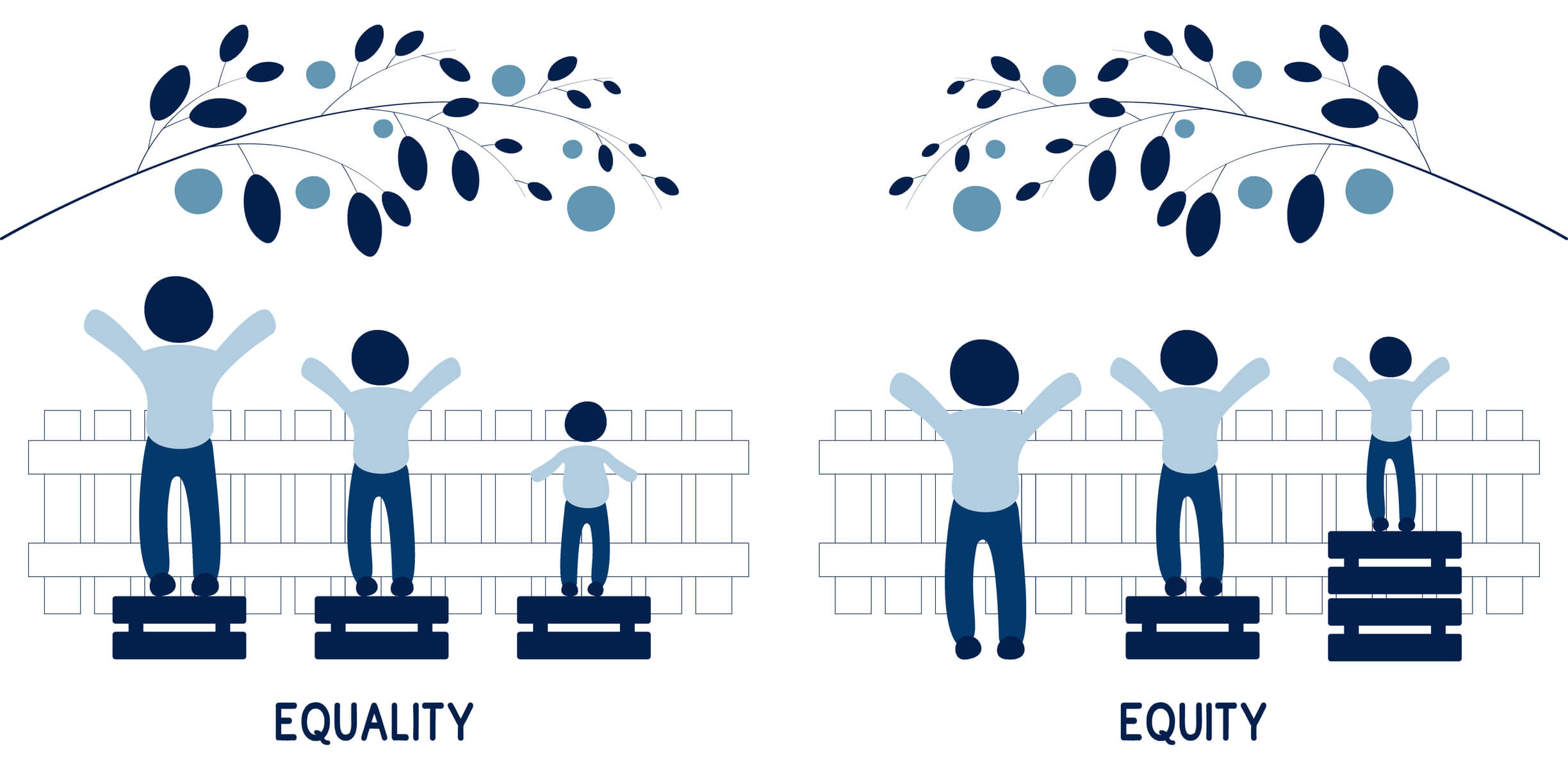
Explore the crucial distinction between providing equal care versus equitable care within emergency medical services (EMS). We give you an in-depth discussion with Ritu Sani
Dr. Avery McKenzie interviews Dr. Eric Adler, regional medical director for Flight for Life, about the challenging and rare procedure of field amputations. They discuss