


Dr. Wright joins us to discuss acute respiratory distress syndrome (ARDS). There has been a lot said about ARDS recently given some of it’s similarities to the COVID-19 disease process. That being said ARDS has been around for a long time and is very much its own disease process. We discuss how to define it, how to recognize it, and how we treat it.
Let’s start with the anatomy-
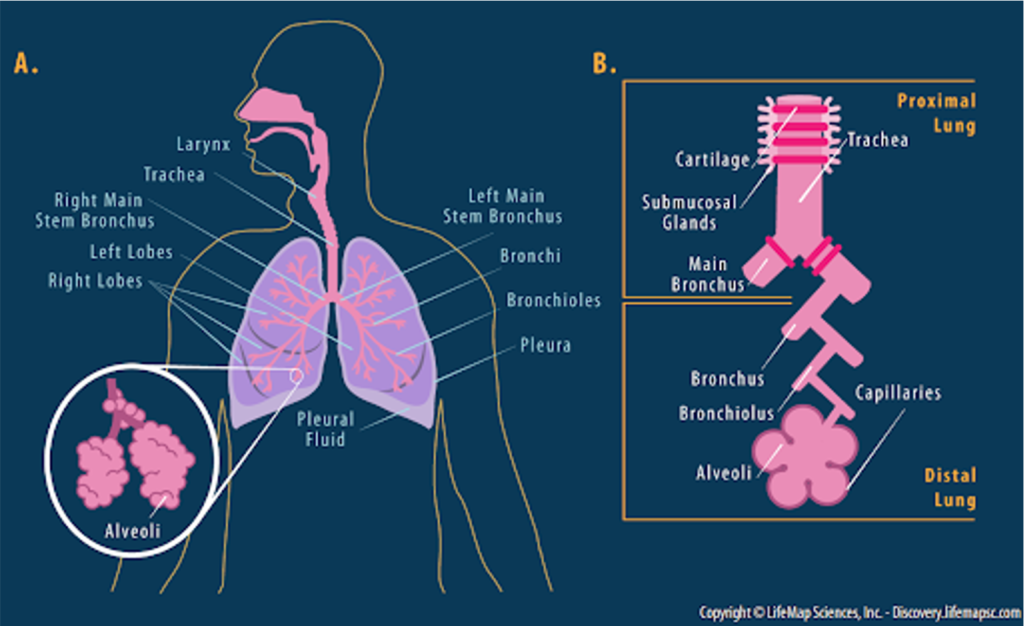
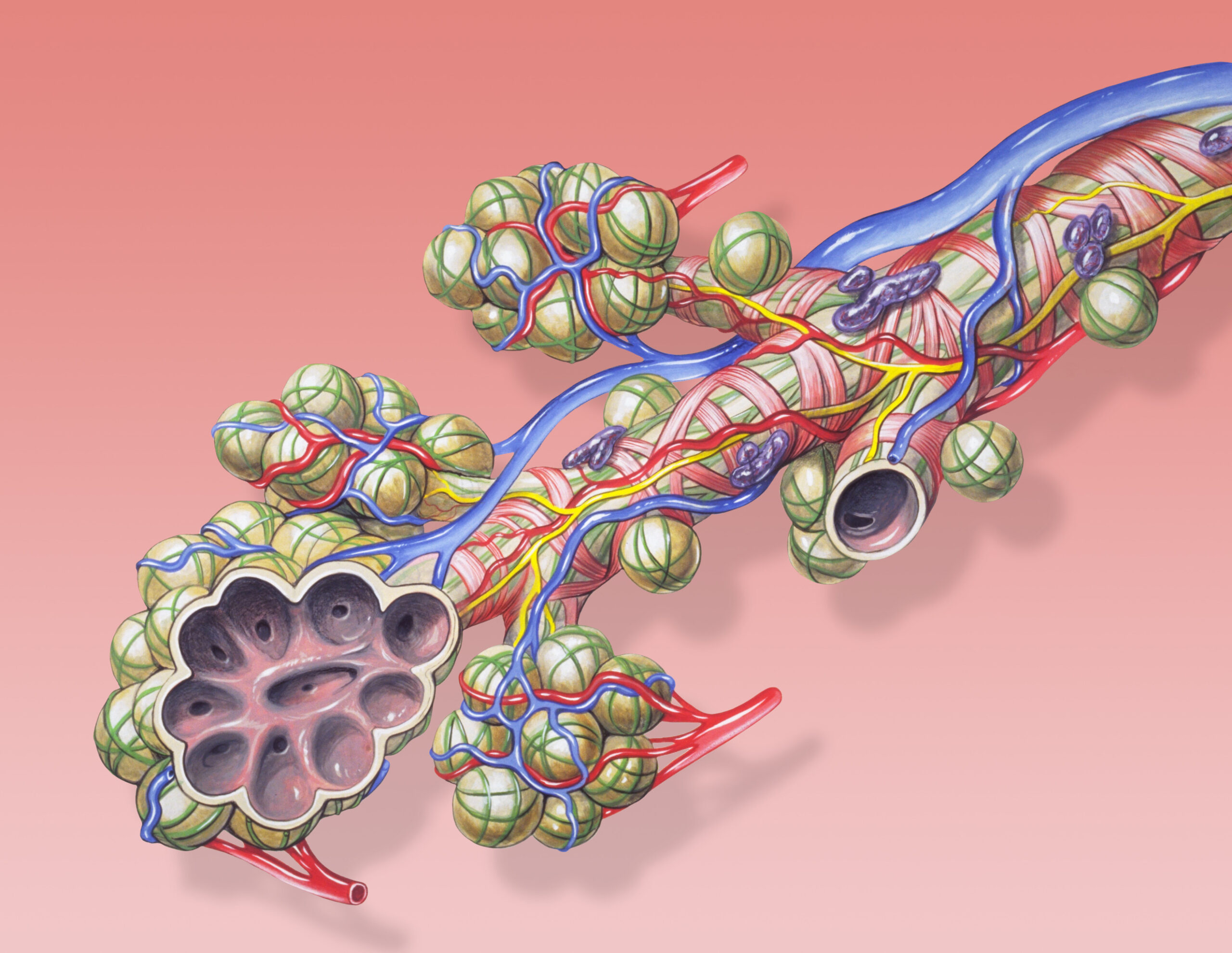
When we think of the airway, we typically think of the more macro picture- the nose, mouth, trachea, bronchi. But let’s remember that the airway physiology is quite complex and incredibly elaborate. If we work our way through the path that oxygen takes, it starts in the larynx, travels through the trachea, and then into the bronchi. The bronchi then further divide into the bronchioles, which divides then become the alveoli. The very thin, single-cell layer alveoli interface with the capillaries to participate in gas exchange – so remember oxygen is crossing through the cell layer form the alveoli to the capillaries, to then join the pulmonary circulation and be transported to the body.
Similarly, the capillaries are offloading their CO2 into the alveoli, which then works its way “backwards,” through the bronchioles, the bronchi, the trachea and the larynx. Take a second to just envision from you’re a/P days this path that oxygen takes, it is going to help when we start talking about how things go wrong.
So we just covered what should happen, the “normal.” Now let’s talk about the abnormal.
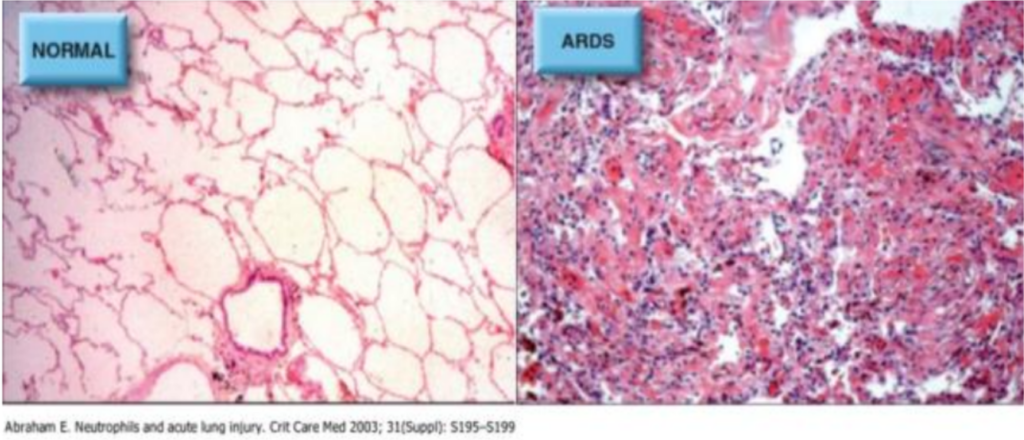
- The picture above shows normal lung tissue vs ARDS lung tissue under a microscope. I encourage you to look at that- it really helps you picture what we are talking about
- The image on the left is normal lung tissue at the alveolar level. You can see those nice thin cells, that capillary interface that requires very little work for an oxygen particle to move from point A to point B.
- Now look at the image on the right. This is what severe ARDS looks like. You can see there is an insane amount of infiltration of inflammatory cells (the purple dots) as well as proteinaceous material that is filling the normal lung tissue- you can imagine that if an O2 particle where to try and get “across” any of this, it will prove particularly challenging.
Remember, there are different things that can cause respiratory failure- this can by a problem with OXYGENATION or a problem with VENTILATION.
- Problems with OXYGENATION occur when there is difficulty delivering oxygen to the organs throughout the body because of problems with the distal airways- issues getting oxygen into the capillaries and successfully delivering them throughout
- Problems with VENTILATION refer to issues in mechanically moving oxygen into the distal areas, and mechanically removing CO2
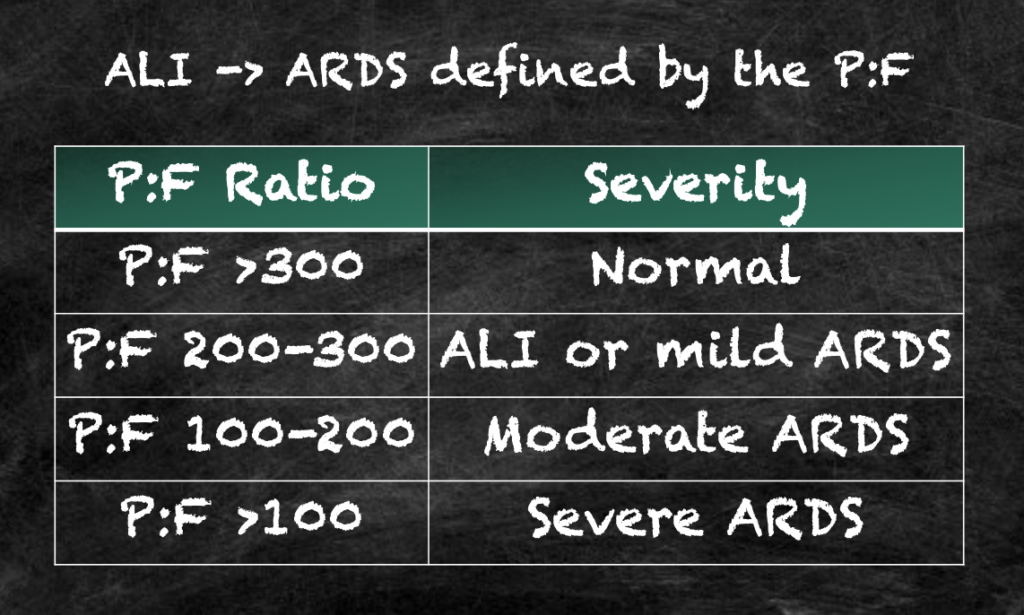
- When we are talking about problems with oxygen delivery to the organs, there are a number of different ways this can go wrong- specifically, how much oxygen is getting into the lungs, how efficiently the gas exchange is occurring at the level of alveoli, and how well the blood is moving through the lungs to receive the oxygen. There are a number of very complex math equations that describe these different ways that oxygen delivery to the tissues can be insufficient, but for the sake of a COVID focus and ARDS, we are going to review something called the P:F ratio.
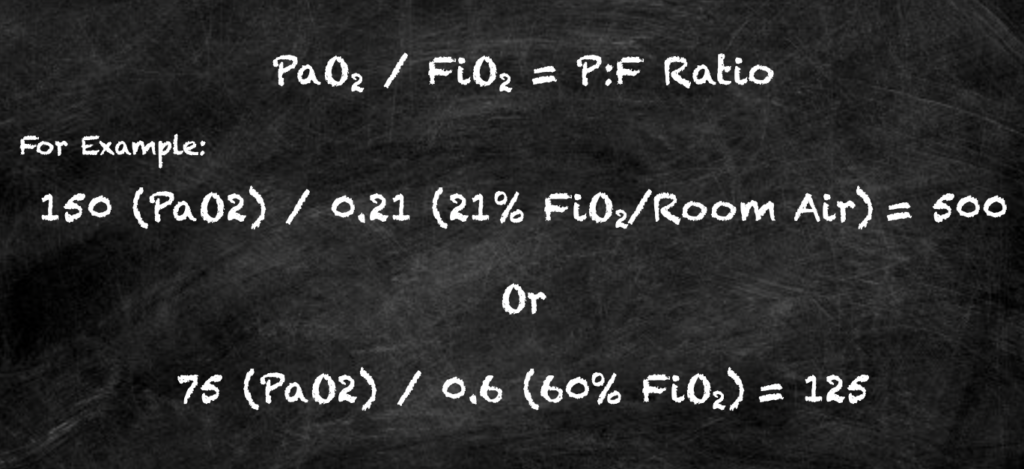
The P:F ratio is the PaO2:FiO2 ratio. This is the ratio of arterial oxygen partial pressure (i.e. if you take a sample of arterial blood, how much oxygen is in there), compared to the FiO2, or the fractional inspired oxygen, meaning the fraction of O2 that is in the lungs, or how much oxygen you are delivering to the alveoli.
- So you are looking at what you are trying to get into the blood, and how much actually makes it there with this figure
- It is used as a clinical indicator for hypoxemia, meaning that if the P:F ratio is LOW, that would indicate severe lung injury.
- Let’s dissect that a little more: If you are delivering a HIGH FiO2 (meaning you are giving someone a significant amount of supplemental oxygen, be it via a ventilator or NRB or BiPAP), but when you measure the oxygen in the blood and it is LOW – This would give us a high denominator and a smaller numerator, thus a lower ratio, indicating there is a problem getting the oxygen that you are trying to get from the lungs to the blood
Now for some definitions:
- ALI is acute lung injury- this is an acute phase of this process, and is defined as a P:F ratio of <300 (meaning there is a proportionally lower amount of oxygen in the blood than there should be)
- On XR, the patients have bilateral infiltrates that look like pulmonary edema, or COVID
- ARDS is Acute Respiratory Distress Syndrome
- This is also acute onset, and the P:F ratio is <200, so even more of a discrepancy between the inspired oxygen and the oxygenation that makes it into the arterial blood system
- This additionally will have bilateral infiltrates c/w pulmonary edema, or COVID
- Both of these definitions also include the caveat that this low P:F ratio CANNOT be explained solely by heart failure, which can cause a similar issue in these numbers
Treatment
- The goal here is “lung protective” ventilation
- We are using an ideal body weight with low tidal volumes and high PEEP (or positive end expiratory pressure) to try and combat that physiology that we just went over.
- The goal is to “push” through that crap in the alveoli, maintain oxygenation, and not cause barotrauma, i.e. not “pop” a lung with aggressive ventilatory settings
- A few other important things for treatment here, some of which apply to the EMS world
- The goal is to have these patients fluid neutral if not a little net-negative, or dry
- So without obvious HYPOVOLEMIA clinically, be VERY CAREFUL giving these patients fluids. The last thing that the lungs need a bunch of extra isotonic fluid to further fill those alveoli and further impair gas exchange
- Finally, if you work in the hospital setting, you may hear about “proning” these patients This means turning them onto the stomachs, as opposed to the classing “lying on their back in the ICU bed” look
- Proning is not something done casually, as you can imagine it requires and immense amount of technical coordination, special beds, protecting the airway, etc to do properly. Further more the data on it has only shown to be helpful in the sickest ICU patients when they are proned for >16 hours. Paper on prone positioning: https://www.nejm.org/doi/full/10.1056/nejmoa1214103.
- So probably not advised in the back of the ambulance. But for your knowledge we have included the following to explain why we prone in the hospital.
- Switching to the prone position can improve gas exchange in the ARDS patient
- It uses gravity to divert blood AWAY from the poorly aerated lungs in the posterior thorax, and increased blood flow to the anterior thorax, where the aeration is better
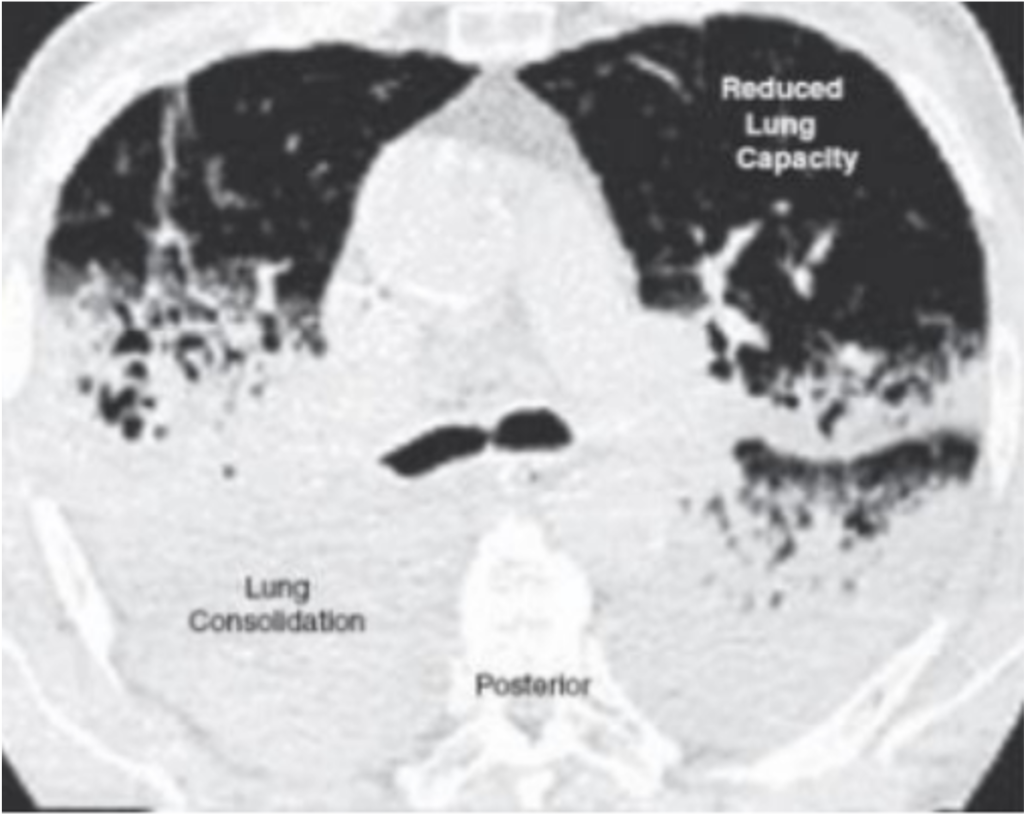
- As the patient is lying on the back for a long time in the ICU, gravity pulls the fluid to the posterior aspect of the lungs, the part that is closest to the bed.
- This leaves very little lung tissue to actually participate in gas exchange as the fluid all settles to the back.
- But remember- blood is a fluid too. So it is ALSO going to the posterior aspect of the lungs because of, well, gravity. So there is more blood flow going to the part of the lungs that is all full of crap.
- There is really no point in blood flowing to this part of the lungs- it cannot get much oxygen from them.
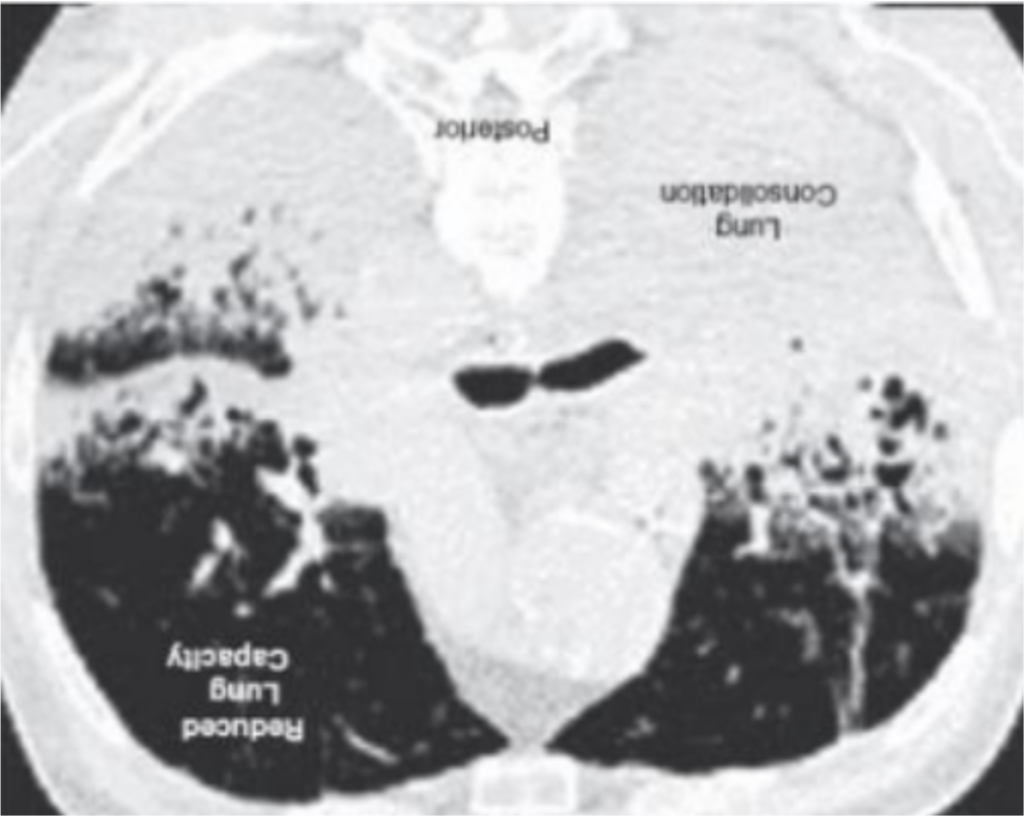
- So now, the are lying on their belly. The crap is still at the back of their lungs, but we are using gravity to pull the blood to the part of the lungs that actually work, improving the ability to get oxygen into the blood stream.
- Thus you can picture if someone is placed on their stomach, the blood flow will improve to these happy parts of the lungs
- In the hospital we actually will sometimes have people with ARDS, especially in the COVID era- self prone. IF they can tolerate it- lie on their stomachs to improve blood flow, and thus oxygen delivery, to the good part. Anecdotally some have reported this being helpful but again there is no data to support this.
Want help turning ARDS physiology into confident care?
Want to get better at connecting respiratory physiology to your next move? Inside the Loud & Clear Fellowship we practice translating physiology into EMS decisions when the patient is sick and the clock is loud. This article explains the concepts. The Loud & Clear Fellowship helps you practice applying concepts like these to real calls, so the next step is grounded in physiology instead of guesswork.
