

Understanding Wide Complex Tachycardia
A wide complex tachycardia (WCT) is a cardiac condition characterized by a rapid heart rate together with a wide QRS complex on an ECG. This condition demands prompt recognition and understanding of safe management principles. This blog post will walk you through our approach to these patients and at the very bottom you will find the approach visually laid out in a diagram and multiple practice examples highlighting many of the points in this discussion.
The Approach to WCT
The complexity of managing WCT lies in not missing the dangerous mimics and distinguishing between ventricular tachycardia (VT) and supraventricular tachycardia (SVT) with aberrancy with each having potentially differing treatment options. At its core is a strategic approach that should take no longer than 30s and doesn’t rely on pinpointing the exact arrhythmia type but rather on understanding the safety and dangers of each treatment option while arriving at a 70% solution. This philosophy, as highlighted by Dr. Kevin Butler in our comprehensive discussion on the subject, rests on having an approach that eschews complete certainty in favor of readiness.
Understanding the Heart’s Conduction and Defining WCT
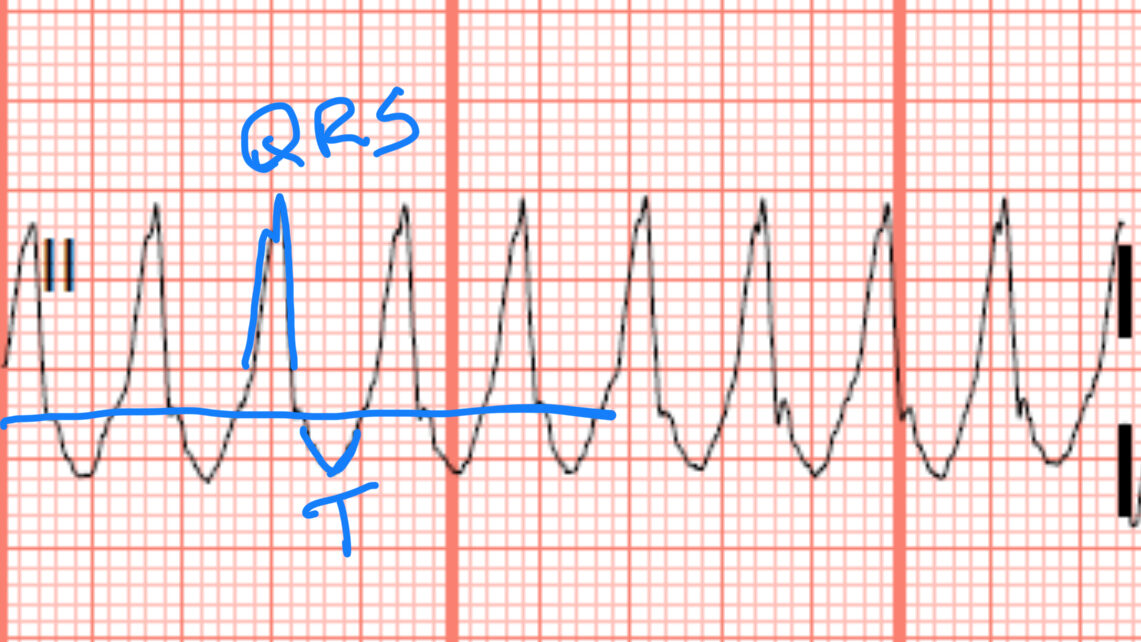
The conduction system transmits electrical impulses within the heart. A WCT is identified when the duration of the QRS complex exceeds 120 milliseconds and the heart beats faster than 100 beats per minute. The causes of a wide complex QRS are various and include bundle branch blocks, medication effects, and notably, ventricular origin of the impulse such as in VTAC.
The QRS duration represents the point of first ventricular cell electrical activation to the last ventricular cell activation.
In a normal functioning conduction system, the electrical activity originates from the SA node, travels down the atria to the AV node and then travels throughout both ventricles nearly simultaneously using the bundle branches. When the ventricular impulse does not utilize the bundle branches it must travel cell to neighboring cell to make it’s way throughout the ventricular (think of someone starting the wave in a football stadium). This takes more time and leads widening of the QRS.
This can occur because one of the bundle branches are blocked or because the electrical impulses are originating in a single ventricular myocyte out side of the bundle branches as in ventricular tachycardia or WPW with abbarency. It can also occur because of certain medication overdoses or electrolyte abnormalities which slow conduction through the cells such as in sodium channel blockade or hyperkalemia.
The SPAM Filter: Don’t miss the mimics
When evaluating WCT, the first step is to rule out major mimics to ventricular tachycardia, remembered by the mnemonic SPAM:
- Sodium channel blockade:
- Certain overdoses such as TCAs, benadryl, or cocaine can lead to a sodium channel blockade within the myocardium causing a wide QRS tachycardia. This can be identified by a combination of history and EKG findings. Typically EKG findings are tachycardia, wide QRS, prolonged QT, and they often have a tall terminal R wave in AVR and right axis deviation. Typically the QRS widening is not as wide as ventricular tachycardia which will normally be >140ms where as sodium channel blockade is usually between 110-140ms. The treatment for this is bolus’s of sodium bicarb until the QRS narrows.
- https://litfl.com/wp-content/uploads/2018/08/ECG-TCA-overdose-Sodium-Channel-Blocking-Agent-Toxicity.jpg
- Potassium imbalance:
- Severe hyperkalemia influences the heart’s conduction similar to a sodium channel blocker but with some unique EKG differences. Again identification will be a combination of history and EKG. Usually these patients will be bradycardia and tachycardia is less common in these patients but can happen if it is seen early or there is another underlying issue such as sepsis. Early EKG findings may include peaked T waves (although this finding does not have good interrater reliability). Later you will see the QRS start to broaden and the QT prolong. Finally a sinusoidal pattern late in the disease process.
- https://www.powerfulmedical.com/wp-content/uploads/2025/01/hyperkalemia-ecg-1-1024×512.webp
- Acute Myocardial infarction:
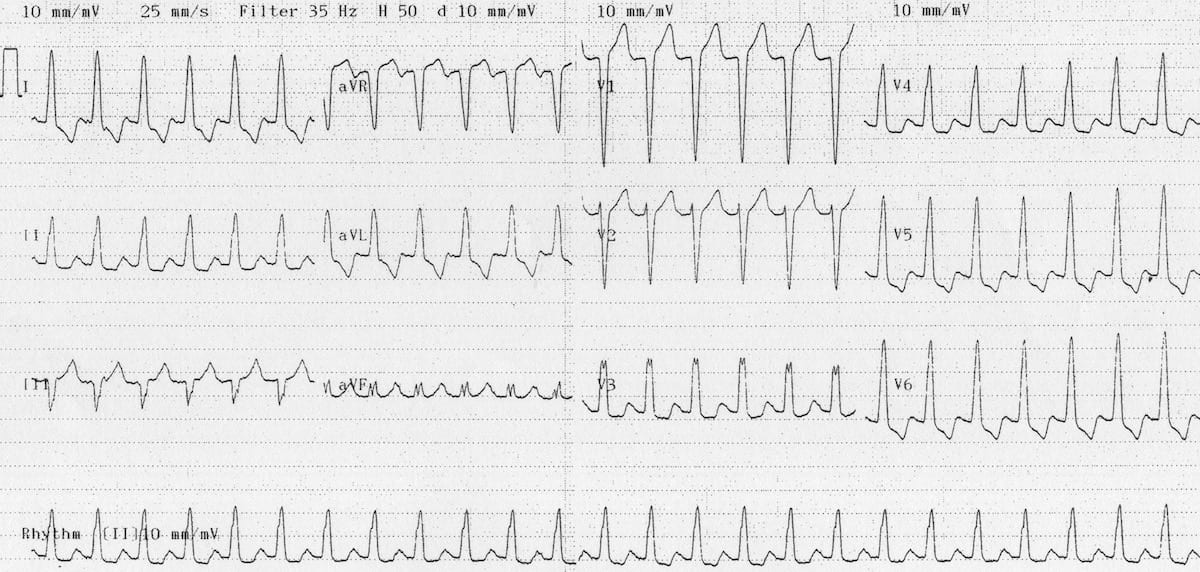
- Massive infarctions can mimic a WCT due to QRS and T wave fusion. Key here is to look at the entire 12 lead. The leads without marked ST elevation will often allow you to identify that the QRS is actually narrowing and what you are mistaking for a wide complex is actually just fusion of the QRS and tombstone T waves.
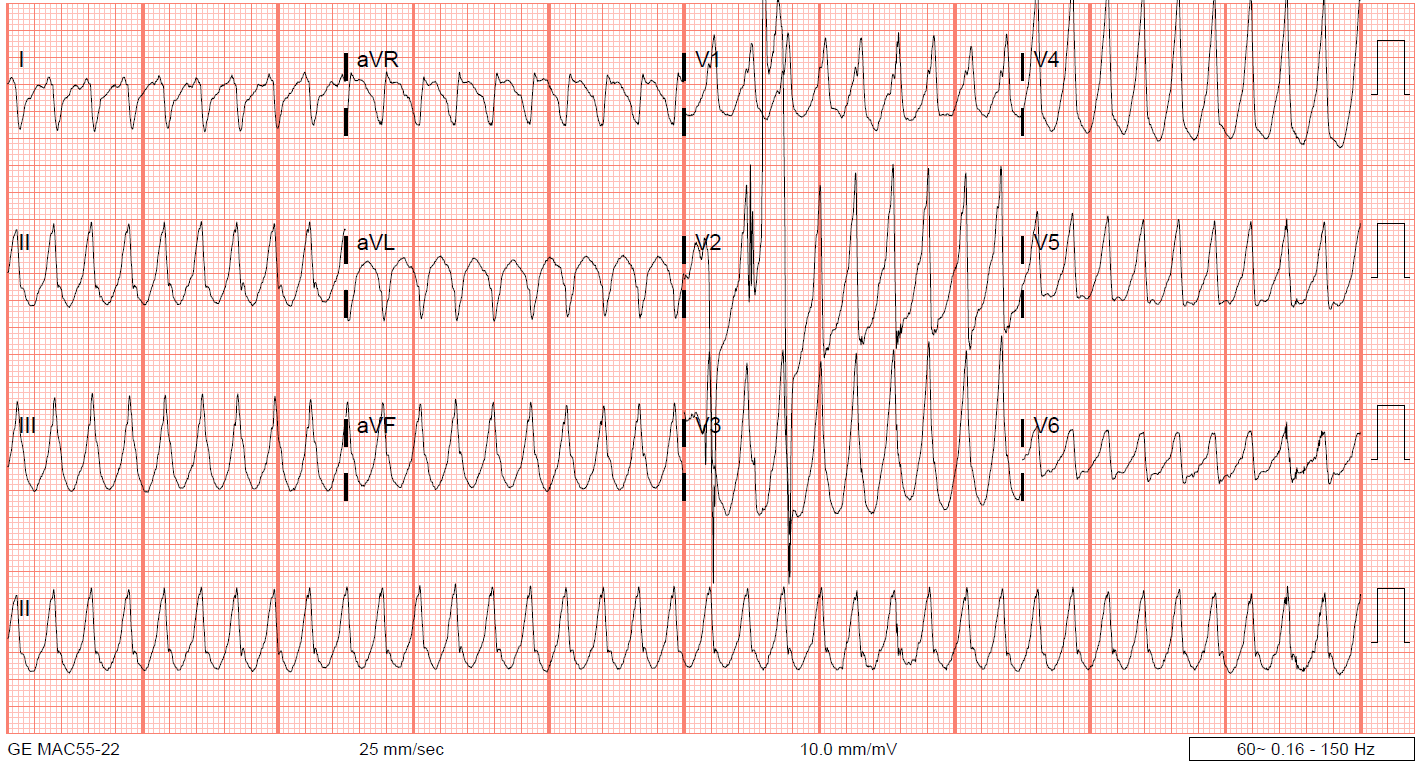
- Notice that in the example below, V1 and III, we can see that the QRS is not actually wide. What gives the appearance of a wide QRS is a massively elevated ST segment that “fuses” the QRS and T wave. These waves are called “shark fin” waves, and in this case are indicative of a massive LAD occlusion
- https://ekgdx.com/blog/vt-vs-svt-with-aberrancy
Want to get more comfortable making decisions when the ECG is not obvious? Inside the Loud & Clear Fellowship we practice the move from pattern recognition to safe action when the call lives in the gray zone.
Assessing Patient Stability
Initial assessment always focuses on patient stability. Stability dictates the urgency and type of intervention, with immediate cardioversion being the course of action in unstable patients who otherwise do not have any evidence of a wide complex tachycardia mimic with the SPAM filter. With these mimics ruled out electricity will safely treat the remainder of our differentials below. Unstable wide complex tachycardia->SPAM filter negative->immediate synchronized cardioversion.
Look for Irregularity
If the SPAM filter is negative and the patient is otherwise stable, next assess for regularity: The majority of the time wide complex tachycardia with irregularity indicates atrial fibrillation with rapid ventricular response and a bundle branch block. But you must also consider rapid atrial fibrillation with pre-excitation (such as WPW) or even torsades de pointe (although these patients are unlikely to be stable). The faster afib is the more subtle the irregularity becomes. You may need to march out multiple R-R intervals with calipers or marks on a second piece of paper to detect the subtle irregularity.
Atrial fibrillation with Pre-Excitation
This is important to identify because some of the treatments we may consider for stable wide complex tachycardia such as amiodarone or adenosine block the AV node. In rapid afib and pre-excitation, there is an abnormal bridge of tissue allowing for the conduction of impulses to the ventricle without the use of the normal conduction pathway. But with a functional AV node, there is still some limit to how quickly these conductions can be transmitted due to the refractory period. The AV node is still applying some brakes. If the AV node is blocked then there is no limit to how quickly this electrical activity can be transmitted across the bridge to the ventricular myocytes and this could potentially lead to lethal decompensation of the rhythm to ventricular fibrillation. So identifying irregularity is key to safely treating these patients and is the next step in our approach after the SPAM filter and determining stability.
EKG findings that can help delineate rapid afib with pre-excitation vs rapid afib with a bundle branch block: if you’re looking at an EKG and have an irregularly irregular rhythm with wide complexes- those complexes are consistent with either a right bundle branch block or a left bundle branch block, the overall rate is under 200, every QRS looks the same as every other QRS, and that patient’s looking pretty stable, that is highly unlikely to be a rapid afib with pre-excitation.
P Waves
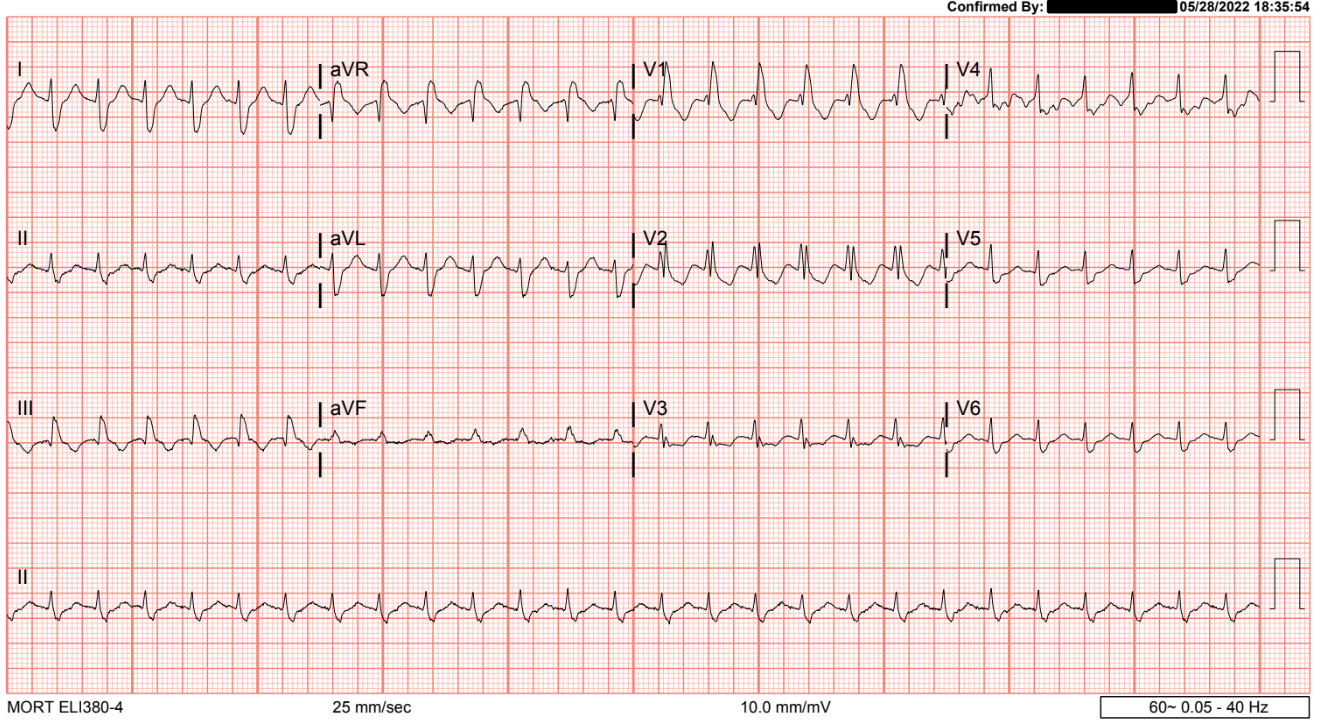
The final step before we move onto our ABCD approach is to check for P waves. A visible P wave before every QRS means the electrical conduction originating above the AV node. A stable wide complex regular tachycardia with p waves before every QRS is either sinus tachycardia with abarrency or atrial flutter with abbarrency. In both instances, we will treat the underlying disease that is causing the tachycardia and need for increased cardiac output. In the instance of atrial flutter if there does not otherwise appear to be an underlying disease driving a compensatory tachycardia we may consider rate control medications in the ED but this is unlikely to be necessary in the prehospital setting.
Sinus tachycardia with p waves visible most clear in leads 1-3 and avf
It’s Probably VT…
If you have made it this far down the algorithm (SPAM filter negative, stable patient, regular rhythm, no identifiable P waves before every QRS), then you are dealing with either ventricular tachycardia (VT) or supraventricular tachycardia (SVT) with aberrancy. A safe approach is to just treat all of these as VT. The reasoning behind this is that the treatment for VT will also treat SVT (the reverse is not true), VT is much more life threatening, the majority of these patients (>80%) will be VT and not SVT with aberrancy (if you add in a patient who has a history of prior MI or cardiomyopathy the probability of VT goes up to 90%). You have 3 options when it comes to prehospital treatment for a stable wide complex regular tachycardia presumed to be VT:
- Do nothing
- If your transport time is short and the patient is otherwise very stable. You may chose to do nothing until the ED. In fact, in the emergency department, if the patient is stable the emergency physician will often consult cardiology for assistance in evaluating the EKG and recommendations on their preferred treatment as they will ultimately be admitting and caring for the patient upstairs.
- Amiodarone or procainamide
- Synchronized Cardioversion
If the patient is stable and you do wish to dive deeper to determine if this is VT vs SVT with aberrancy we do not recommend any of the established criteria. The current established criteria such as the brugada criteria are difficult to memorize, take at least 90 seconds to apply when we recommend taking no more than 30 seconds in these patients before determining how you will treat, and they do not have 100% specificity so they may still lead you to miss VT. Instead, we recommend a simple approach based on physiologic principles and the mnemonic ABCD so that onerous memorization and recall are not needed in these stressful situations.
The ABCD Approach: Beyond Basics
A: Axis
A normal electrical impulse starts in the sinus node, moves through the AV node, and travels from the heart’s upper right to lower left.
- Extreme axis deviation (more than -90°) suggests VT.
- Look at lead AVR: a monomorphic upright QRS is a red flag for extreme right axis deviation and VT.
B: Bundle Branch Block Patterns
Wide QRS complexes in SVT with aberrancy often resemble a typical right or left bundle branch block (BBB).
- Examine leads V1, V6, and I:
- Right BBB: Positive QRS in V1, slurred S in V6 and I.

- Left BBB: Negative QRS in V1, broad/notched R in V6 and I.

- If the QRS pattern doesn’t align with a normal bundle branch block pattern, suspect VT.
C: Concordance
Concordance refers to whether QRS complexes in the precordial leads (V1–V6) all point in the same direction.
- Positive or negative concordance across all leads suggests a ventricular origin of the rhythm.

D: Duration
QRS width provides a vital clue: if QRS duration >160 ms, it’s most likely VT
- SVTs with BBB still leverage bundle branch conduction fibers to half the heart that aren’t blocked, resulting in slightly less delay.
- VT lacks this advantage relying purely on cell to cell conduction, often leading to wider QRS complexes (>160 ms).
When to Treat as VT
- If any of the ABCD criteria suggest VT, it’s almost certainly VT. Treat as VT with one of the three options described above.
- Even when all criteria are unremarkable, the possibility of VT still cannot be ruled out.
- But there’s no definitive evidence that you’re not dealing with an SVT with aberrancy
- You may give a trial of adenosine.
- If they convert with this, then this was SVT with aberrancy.
- If not, then this is VT. Proceed with VT treatment.
EMS Treatment Considerations
What Not to Do
- Never administer beta blockers or calcium channel blockers (e.g., diltiazem) when VT is on the differential.
- These drugs can worsen instability in ventricular rhythms.
Safe Approaches
- Electricity Is Your Friend:
- Synchronized cardioversion is safe and effective for unstable or concerning rhythms.
- We recommend starting at 200 J biphasic if protocols allow.
- Medications:
- Amiodarone: Effective for VT and safe in SVT with aberrancy.
- Adenosine: In regular, stable wide complex tachycardia, it’s diagnostically useful and safe—even in VT.
- Sedation/anxiolysis in Cardioversion:
- If time permits, administer anxiolysis (e.g., midazolam) for patient comfort. If the patient is unstable, prioritize electricity over sedation.
Key Takeaways
- Stability First: Shock unstable patients immediately. Stability is the foundation of all decisions.
- Structured Approach: Use the SPAM filter, assess irregularity and P waves, and employ the ABCD mnemonic to refine your interpretation.
- Be Comfortable with Uncertainty: When in doubt, treat as VT—it’s the safest default.
- Practice ECG Interpretation: Familiarity with ECG patterns and systematic practice is key to confident decision-making.

Want help building this judgment before your next hard rhythm call?
This article gives you the framework. The Loud & Clear Fellowship gives you repeated practice applying frameworks like this to realistic EMS cases, so uncertainty turns into a clear next step.
